🚭 Best Treatments for Tobacco Addiction in the Elderly
 Tobacco use in older adults—whether smoked (cigarettes, bidis, cigars) or smokeless (paan, khaini, gutkha)—requires a gentle but structured approach, considering physical comorbidities, cognitive limitations, and psychological dependency.
Tobacco use in older adults—whether smoked (cigarettes, bidis, cigars) or smokeless (paan, khaini, gutkha)—requires a gentle but structured approach, considering physical comorbidities, cognitive limitations, and psychological dependency.
🔁 The Use-Abuse-Dependence Cycle & Allostasis
Tobacco addiction is a progressive illness:
- Use: Initially for pleasure, curiosity, or social inclusion
- Abuse: Continued use despite early signs of harm (cough, throat irritation, family concern)
- Dependence: Psychological and physiological need to avoid withdrawal, not to enjoy
This cycle is underpinned by allostasis—the brain’s adaptation to frequent nicotine stimulation. Over time, the brain recalibrates its ‘normal’ functioning around nicotine. This leads to:
- Increased baseline stress without nicotine
- Decreased reward from natural activities (food, conversation)
- Compulsive use driven by avoidance of discomfort rather than pleasure
In the elderly, this cycle is often decades old—deeply entrenched, automated, and normalized.
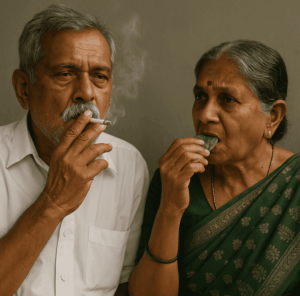
👩🏽🌾 Smokeless Tobacco in Elderly Women – The Hidden Epidemic
In rural and semi-urban India, elderly women frequently use smokeless tobacco (e.g., betel quid, khaini, mishri, tobacco toothpaste):
- Culturally accepted
- Often linked to oral hygiene or digestive aid myths
- Used secretly due to gender norms
Health consequences include:
- Oral cancers, gum recession, leukoplakia
- Nutritional deficiencies due to altered taste and appetite
- Dependency with severe withdrawal symptoms (headache, irritability)
Targeted education, oral screening camps, and community support are crucial for addressing this neglected group.
🔹 1. Nicotine Replacement Therapy (NRT)
NRT helps reduce withdrawal symptoms by delivering controlled nicotine without harmful smoke or chemicals.
- Options and Comparison:
- Nicotine Gum
- Use: Chew and park method, suitable for active users.
- Challenges: Not ideal for those with dentures, TMJ pain, or poor dental status.
- Indian Brands: Nicotex Gum, NicoChew, KwikNic.
- Nicotine Lozenges (Pastilles)
- Use: Slowly dissolves in the mouth, no chewing needed.
- Best for: Smokeless tobacco users and those with dental issues.
- Indian Brands: Nicotex Lozenge, NicoMeltz, QuitSure Pastilles.
- Nicotine Patch
- Use: Transdermal delivery over 16–24 hours.
- Pros: Steady release; good for those with routine compliance.
- Cons: May cause skin irritation, less flexible with dose titration.
- Indian Brands: Nicotex Patch, Nicogum Patch.
- Inhalers and Nasal Sprays
- Less commonly used in elderly due to dexterity issues and cost.
- Nicotine Gum
- Best for: Gradual weaning, especially when combined with behavioral support
- Caution: Monitor for skin irritation (patch), jaw issues (gum), and medication interactions
🔹 2. Non-Nicotine Medications
Bupropion SR (Zyban / Wellbutrin)
- Originally an antidepressant, also reduces cravings and withdrawal
- Useful if depression is a coexisting concern
- Start low, go slow in elderly
- Avoid in patients with seizure risk or underweight status
Varenicline (Champix)
- Partial agonist at nicotine receptors – reduces pleasure from smoking and cravings
- Superior quit rates in clinical trials
- Effective but caution in elderly with renal impairment or psychiatric history
🔹 3. Behavioral Support and Counseling
- Brief Interventions: 3–5 minutes of advice increases quit rates
- Motivational Interviewing: Helps shift the mindset from fatalism (“why bother now?”) to hope (“I want to breathe better”)
- Structured therapy: CBT for triggers (e.g., loneliness, boredom)
- Family involvement: Key for success—especially helping replace rituals
🔹 4. Smokeless Tobacco – Specific Interventions
Smokeless tobacco (gutkha, pan masala, khaini) is often seen in rural/working-class elderly, with a deep-rooted cultural angle.
- NRT lozenges or gum may be better accepted
- Counseling focused on oral health, dental effects, and social stigma
- Regular oral screening for leukoplakia, submucous fibrosis
- Peer support groups in local language helpful
🔹 5. Technology-Assisted Support
- Telepsychiatry and digital deaddiction consults
- Mobile apps with daily tracking and motivational messages
- Support from community health workers for follow-up in low-literacy populations
🧘🏽♂️ Smoking Refusal Skills and Alternate Techniques
- Refusal Skills for Social Situations:
- “No thanks, I’m quitting for my health.”
- “Doctor advised me to avoid it—it’s affecting my breathing.”
- Role-play common triggers and responses with family/friends
- Urge Surfing:
- Practice riding out the craving like a wave—it rises, peaks, and fades
- Encourage using a timer or stopwatch to observe duration of the urge
- Deep breathing or sipping water during cravings can be helpful
- Alternate Coping Techniques:
- Clove chewing, fennel seeds, or sugar-free gums
- Keeping hands and mouth busy—e.g., knitting, puzzles, rosary beads
- Daily routines: Morning walk, music, TV shows, gardening
- Replacing cigarette breaks with social calls or light stretches
🧠 Additional Tips:
- Rule out underlying depression, grief, or dementia, which may worsen dependency
- Watch for polypharmacy interactions
- Reinforce the message: “It’s never too late, and you’re never too old to quit.”
🩺 Need Help? Meet Dr. Srinivas Rajkumar T
If you or your loved one is struggling with smoking or tobacco use in older age, consult with:
Dr. Srinivas Rajkumar T, MBBS, MD (Psychiatry)
Consultant Psychiatrist – Geriatric and Addiction Psychiatry
Apollo Clinic, Velachery – Chennai
📍 27/17 Velachery Road, Nagendra Nagar, Velachery, Chennai, Tamil Nadu 600042
📞 Call: +91 85951 55808
🌐 Visit: www.srinivasaiims.com
🕐 In-person & teleconsultation available by appointment
Get compassionate, evidence-based care for a better tomorrow.