Lumateperone: A New-Generation Antipsychotic That Rewrites Old Assumptions
 For decades, antipsychotic development followed a familiar trade-off:
For decades, antipsychotic development followed a familiar trade-off:
control psychosis at the cost of metabolic, motor, and endocrine side effects.
Lumateperone represents a serious attempt to break that bargain—not by being “stronger,” but by being more selective, more integrated, and more neurobiologically respectful.
It is not a revolutionary molecule in the dramatic sense.
It is something subtler—and arguably more important: a convergence drug.
What Is Lumateperone?
Lumateperone (approved as Caplyta) is a second-generation antipsychotic indicated for:
-
Schizophrenia
-
Bipolar depression (both bipolar I and II)
Its clinical interest lies less in its indications and more in how it achieves efficacy with a surprisingly benign side-effect profile.
Mechanism of Action: Why Lumateperone Is Different
Lumateperone does not fit neatly into the “dopamine antagonist” box.
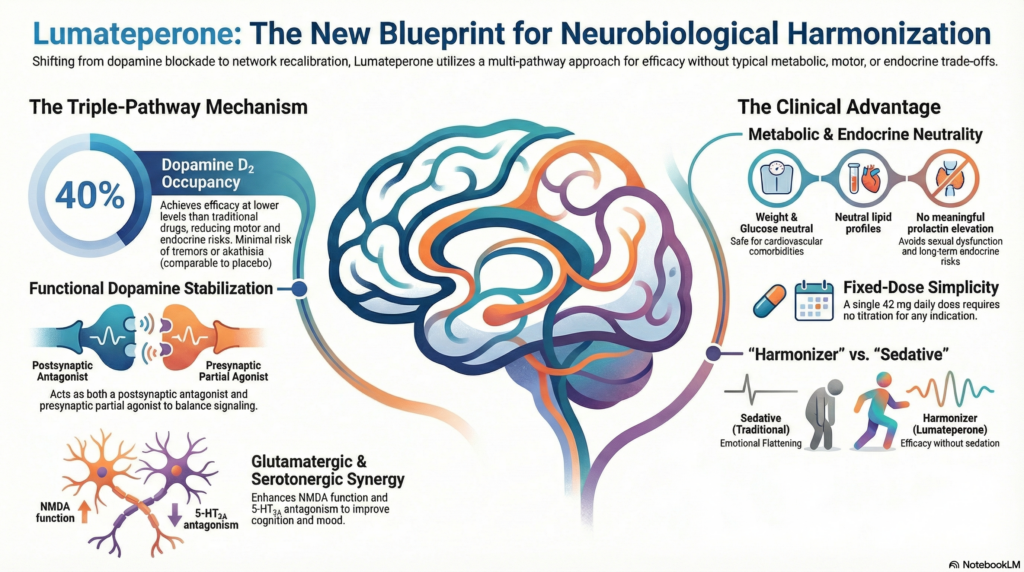
Instead, it operates through three coordinated pathways:
1. Dopamine Modulation, Not Blunt Blockade
-
Acts as a postsynaptic D₂ antagonist
-
Acts as a presynaptic D₂ partial agonist
-
Results in functional dopamine stabilization rather than suppression
Importantly:
-
Effective at ~40% D₂ receptor occupancy
-
Traditional antipsychotics often require >65–70%
This lower occupancy explains:
-
Minimal extrapyramidal symptoms (EPS)
-
Little or no prolactin elevation
2. Serotonin Modulation with Antidepressant Relevance
-
Potent 5-HT₂A antagonism
-
Enhances dopamine release in the prefrontal cortex
This serotonergic effect likely contributes to:
-
Antidepressant efficacy in bipolar depression
-
Cognitive and negative symptom benefits
3. Glutamatergic Downstream Effects
Lumateperone indirectly enhances NMDA receptor function via:
-
Increased phosphorylation of GluN2B subunits
-
Modulation of glutamate signaling balance
This is where lumateperone quietly departs from most antipsychotics and enters territory relevant to:
-
Cognitive symptoms
-
Negative symptoms
-
Mood regulation
Clinical Implications of This Mechanism
Lumateperone behaves less like a sedating antipsychotic and more like a neurochemical harmonizer.
In practice, this means:
-
Antipsychotic efficacy without emotional flattening
-
Mood benefits without switching risk
-
Cognitive neutrality (or mild improvement) rather than impairment
Efficacy: What the Data Actually Shows
Schizophrenia
-
Demonstrated efficacy for positive symptoms
-
Modest but meaningful effects on negative symptoms
-
Functional outcomes comparable to other SGAs
Bipolar Depression
-
Effective as monotherapy
-
No requirement for combination with mood stabilizers
-
No signal for treatment-emergent mania in trials
This is clinically important, especially in patients where:
-
Quetiapine causes metabolic burden
-
Lurasidone causes akathisia
-
Olanzapine is not an option
Side Effect Profile: Where Lumateperone Truly Stands Out
Metabolic Effects
-
Minimal weight gain
-
Neutral lipid and glucose profile
-
No significant insulin resistance signal
Prolactin
-
No meaningful elevation
-
Safe in patients with sexual dysfunction, galactorrhea concerns, or long-term endocrine risk
Extrapyramidal Symptoms
-
EPS rates comparable to placebo
-
Akathisia uncommon
Sedation
-
Mild somnolence in some patients
-
Generally less sedating than quetiapine
In many ways, lumateperone behaves more like a well-tolerated antidepressant with antipsychotic efficacy than a traditional antipsychotic.
Dosing Simplicity
-
Fixed dose: 42 mg once daily
-
No titration required
-
No dose adjustment based on indication
This reduces:
-
Prescribing complexity
-
Early dropouts
-
Anxiety around “dose escalation”
Drug Interactions and Precautions
-
Metabolized primarily via CYP3A4
-
Avoid strong CYP3A4 inducers or inhibitors
-
Caution with alcohol and CNS depressants
No routine lab monitoring is required—another quiet advantage.
Where Lumateperone Fits Best Clinically
Lumateperone is particularly attractive in:
-
First-episode psychosis (where side effects shape long-term adherence)
-
Bipolar depression with antipsychotic sensitivity
-
Patients who refuse or discontinue SGAs due to weight gain or sexual side effects
-
Individuals with medical comorbidities where metabolic neutrality matters
It is not ideal for:
-
Acute severe agitation requiring rapid sedation
-
Treatment-resistant schizophrenia needing high D₂ blockade
A Conceptual Shift: From Blockade to Balance
Lumateperone signals a broader shift in psychopharmacology:
from neurotransmitter suppression
to network recalibration
Rather than overwhelming the dopamine system, it nudges multiple systems—dopamine, serotonin, glutamate—toward a more functional equilibrium.
This approach aligns with modern thinking in:
-
Bipolar spectrum disorders
-
Negative symptoms of schizophrenia
-
Cognitive and affective dimensions of psychosis
Final Reflection
Lumateperone is not a “miracle drug.”
It will not replace clozapine, nor should it.
But it represents something arguably more valuable:
a rethinking of how much receptor occupancy is truly necessary to heal rather than blunt the brain.
In that sense, lumateperone feels less like an endpoint and more like a blueprint for the next generation of psychiatric medications.
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808