Why ADHD Increases Vulnerability to Regression After Trauma: A Developmental–Neurobiological Perspective
 Regression following trauma is often misunderstood as emotional immaturity or personality weakness. In adults with Attention-Deficit/Hyperactivity Disorder (ADHD), this misinterpretation is particularly common. Yet the increased vulnerability of individuals with ADHD to regressive responses after trauma is neither incidental nor psychological in the pejorative sense. It arises from the intersection of neurodevelopmental differences, stress neurobiology, and developmental timing.
Regression following trauma is often misunderstood as emotional immaturity or personality weakness. In adults with Attention-Deficit/Hyperactivity Disorder (ADHD), this misinterpretation is particularly common. Yet the increased vulnerability of individuals with ADHD to regressive responses after trauma is neither incidental nor psychological in the pejorative sense. It arises from the intersection of neurodevelopmental differences, stress neurobiology, and developmental timing.
Understanding this intersection allows a more precise and humane reading of post-traumatic behaviour in ADHD.
ADHD as a Disorder of Self-Regulation, Not of Capacity
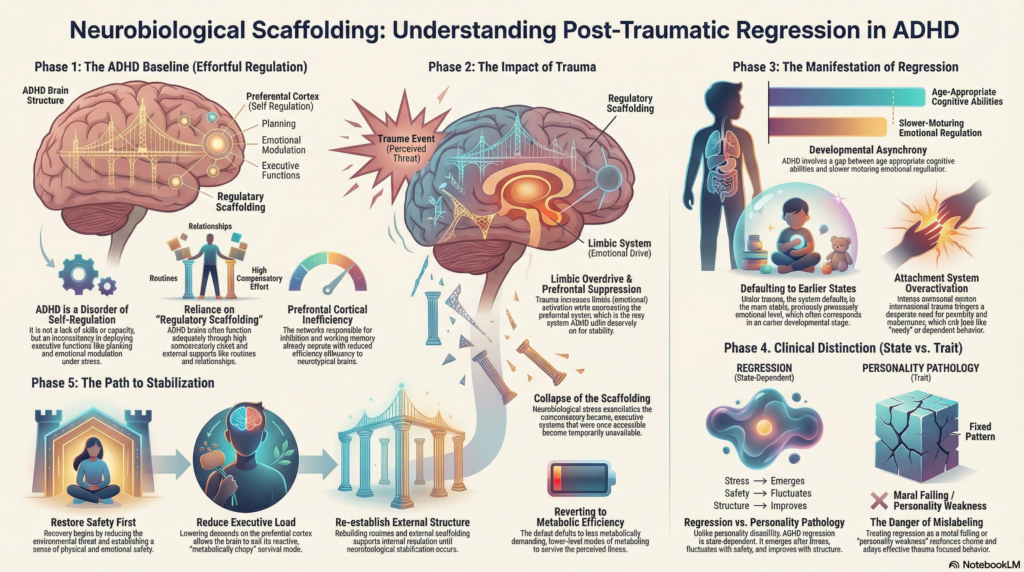
Contemporary models conceptualise ADHD less as a disorder of attention and more as a disorder of self-regulation across time. Individuals with ADHD do not lack skills; rather, they experience inconsistency in the deployment of those skills, particularly under stress.
Executive functions—planning, inhibition, emotional modulation, working memory—are heavily dependent on prefrontal cortical networks that are already operating with reduced efficiency in ADHD. Under ordinary circumstances, these networks function adequately through compensatory effort. Trauma, however, introduces a level of neurobiological stress that overwhelms this compensatory balance.
Regression, in this context, reflects not loss of competence but collapse of regulatory scaffolding.
Stress, Trauma, and Prefrontal Vulnerability
Trauma exerts its effects through well-described neurobiological pathways. Acute or chronic stress increases limbic activation while simultaneously suppressing prefrontal cortical activity. This shift is adaptive in immediate danger but maladaptive when prolonged.
For individuals with ADHD, this stress-induced prefrontal suppression has disproportionate effects. Executive systems that were already effort-dependent become inaccessible. Emotional modulation weakens. Behaviour becomes more reactive and less reflective.
The individual may appear younger, more impulsive, or more dependent—not because of psychological regression in the symbolic sense, but because the brain temporarily reverts to less metabolically demanding modes of functioning.
Developmental Asynchrony and Trauma Reactivation
A defining feature of ADHD is developmental asynchrony. Cognitive abilities may be age-appropriate or even advanced, while emotional regulation and impulse control mature more slowly.
Trauma has a specific tendency to reactivate earlier emotional states and memory networks. When trauma occurs in a person with ADHD, the system tends to default to the most stable and previously successful emotional regulatory level. This level may correspond to an earlier developmental stage.
As a result, the individual may exhibit behaviour that seems incongruent with their intellectual or professional functioning. This mismatch often confuses clinicians and families, leading to moral interpretations of what is in fact a developmentally predictable response.
Emotional Intensity, Rejection Sensitivity, and Attachment Activation
Many individuals with ADHD exhibit heightened emotional reactivity and sensitivity to interpersonal cues. Rejection sensitivity, while not universal, is a common and clinically significant phenomenon.
Interpersonal trauma—abandonment, betrayal, humiliation—activates attachment systems. In ADHD, these systems are often poorly buffered by cognitive modulation. Emotional pain escalates rapidly, and behaviours aimed at restoring connection or safety intensify.
Regression in such cases reflects attachment system overactivation, not manipulation or dependency pathology. The person is attempting to regulate threat through proximity, reassurance, or emotional expression.
Reliance on External Regulation and Its Sudden Loss
Another under-appreciated aspect of ADHD is the degree to which functioning depends on external regulatory supports. Structure, routines, deadlines, feedback, and relationships often serve as stabilising forces.
Trauma disrupts these external regulators. Loss of a relationship, workplace instability, health crises, or sudden change dismantles the scaffolding that supports self-regulation. Internal regulatory mechanisms may not yet be robust enough to compensate, resulting in functional regression.
This phenomenon explains why some individuals with ADHD appear to “fall apart” after life events that others navigate with relative stability.
Regression Versus Personality Pathology
A critical clinical distinction must be made between state-dependent regression and enduring personality traits. In ADHD, regressive behaviours typically:
-
Emerge after identifiable stress or trauma
-
Fluctuate with environmental safety
-
Improve with support and structure
-
Do not reflect pervasive identity disturbance
Mislabeling these responses as personality pathology risks reinforcing shame, delaying trauma-focused intervention, and undermining recovery.
Implications for Treatment and Recovery
Effective intervention requires a recalibration of expectations. Recovery in ADHD following trauma does not occur through confrontation or demands for maturity. It unfolds through:
-
Restoration of safety
-
Reduction of executive load
-
Re-establishment of external structure
-
Gradual reactivation of self-regulatory capacity
-
Processing of traumatic memory
With appropriate support, regression resolves not through effortful “growing up,” but through neurobiological stabilization.
Conclusion
ADHD does not predispose individuals to fragility; it predisposes them to visible dysregulation under stress. Trauma exposes the cost of sustained self-regulatory effort and temporarily renders earlier coping modes dominant.
Seen through a developmental-neurobiological lens, regression in ADHD is neither surprising nor pathological. It is an intelligible response at the intersection of brain development, stress physiology, and lived experience.
Understanding this distinction shifts clinical practice away from judgment and toward precision—and in doing so, improves outcomes for a population that is often misunderstood precisely when it is most vulnerable.
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808