Sleep Studies Can Predict Early Parkinsonism How REM Sleep Behavior Disorder Reveals Parkinson’s Disease Years in Advance
 Parkinson’s disease does not begin with a tremor. That familiar shaking hand is often the final act, not the opening scene. Long before slowness, stiffness, or gait freezing appear, the brain gives subtle warnings—most reliably during sleep.
Parkinson’s disease does not begin with a tremor. That familiar shaking hand is often the final act, not the opening scene. Long before slowness, stiffness, or gait freezing appear, the brain gives subtle warnings—most reliably during sleep.
Modern sleep medicine has uncovered a striking truth:
a properly conducted sleep study can predict Parkinsonism years, sometimes decades, before diagnosis.
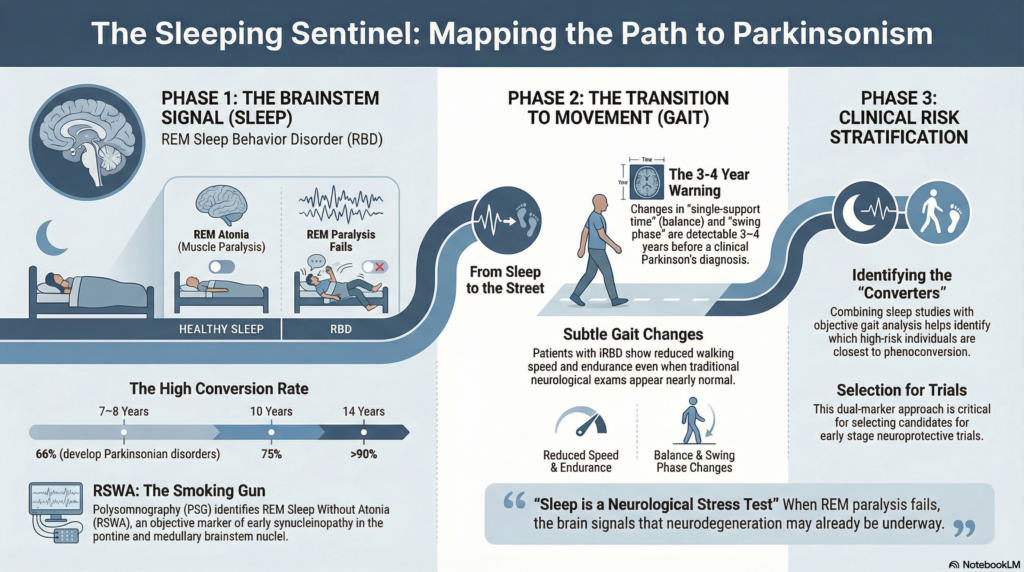
At the heart of this insight lies REM Sleep Behavior Disorder (RBD).
REM Sleep: When the Brain Is Awake but the Body Is Silent
REM (Rapid Eye Movement) sleep is the phase of vivid dreaming. In healthy individuals, the brainstem switches on a powerful safety mechanism: REM atonia—near-complete paralysis of voluntary muscles.
This prevents us from acting out our dreams.
In REM Sleep Behavior Disorder, this paralysis fails.
People may:
-
Talk, shout, punch, or kick in sleep
-
Leap from bed while dreaming
-
Sustain injuries or injure bed partners
This is not psychological stress or “bad dreams.”
It is neurological dysfunction.
Isolated RBD: A Prodromal Neurodegenerative State
When RBD occurs without any diagnosed neurological illness, it is called isolated (idiopathic) RBD – iRBD.
Long-term cohort studies have delivered a sobering but powerful finding:
-
~66% of people with iRBD develop Parkinson’s disease, Dementia with Lewy Bodies, or Multiple System Atrophy within 7–8 years
-
~75% by 10 years
-
Over 90% by 14 years
In clinical terms, iRBD is one of the strongest known predictors of Parkinsonian disorders.
It is not merely a sleep disorder.
It is early synucleinopathy in disguise.
What Does a Sleep Study Actually Show?
A polysomnography (PSG) records brain waves, eye movements, muscle tone, breathing, oxygen levels, and heart rhythm.
In iRBD, PSG demonstrates REM Sleep Without Atonia (RSWA):
-
Persistent muscle activity during REM sleep
-
Loss of the normal motor “off-switch”
This finding is objective, reproducible, and biologically meaningful.
The affected brain regions include:
-
Pontine and medullary brainstem nuclei
-
REM inhibitory motor circuits
-
Cholinergic systems implicated early in Parkinson’s disease
These are among the earliest sites of Parkinsonian pathology.
From Sleep to Movement: Strengthening Prediction With Gait
Sleep studies identify risk.
But can we identify who will convert sooner?
A 2026 Scientific Reports (Nature Portfolio) study adds a crucial layer by examining objective gait changes in people with iRBD.
Key findings:
-
Even before clinical Parkinsonism, iRBD patients showed:
-
Reduced walking speed
-
Reduced walking endurance
-
-
Those who later converted to Parkinson’s disease or Dementia with Lewy Bodies showed:
-
Reduced single-support time (time spent balancing on one leg)
-
Reduced swing phase
-
Increased stance time
-
These changes were detectable 3–4 years before diagnosis, even when neurological examinations were nearly normal.
In simple terms:
Parkinson’s disease announces itself first in sleep, and then in the rhythm of walking.
Why This Makes Neurological Sense
Parkinson’s disease does not start in the hands.
It starts in the brainstem.
Early degeneration affects:
-
REM sleep regulation
-
Autonomic control
-
Gait rhythm and postural timing
RBD reflects loss of REM motor inhibition.
Early gait rhythm changes reflect loss of motor timing and balance confidence.
Together, they form a coherent prodromal signature of Parkinsonism.
Why This Matters in Clinical Practice
Early Identification
Sleep studies allow identification of individuals at very high risk long before motor disability appears.
Risk Stratification
Combining PSG-confirmed RBD with objective gait analysis helps:
-
Identify those closer to phenoconversion
-
Guide intensity of follow-up
-
Select candidates for neuroprotective trials
A Paradigm Shift
Neurology is moving from late diagnosis to early trajectory tracking.
Sleep laboratories are becoming early-warning systems for neurodegeneration.
What Sleep Studies Cannot Yet Do
-
They cannot predict the exact timeline for an individual
-
They cannot reliably distinguish between PD, DLB, or MSA early on
-
They do not replace clinical judgment
But as biomarkers go, few are as strong, consistent, and biologically grounded as RBD.
The Take-Home Message
Sleep is not passive rest. It is a neurological stress test.
When REM sleep loses its paralysis, the brain is quietly signaling that neurodegeneration may already be underway. With modern sleep studies—and complementary tools like gait analysis—we are finally learning to listen.
Parkinsonism often begins in the night.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com
📞 +91-8595155808