Assessment Instruments in Geriatric Psychiatry: Making Sense of Complexity
 Caring for older adults in psychiatry often feels like solving a layered puzzle. Symptoms are subtle, presentations are atypical, and medical conditions frequently overlap with psychiatric ones. In this context, standardized assessment instruments are not optional—they are essential.
Caring for older adults in psychiatry often feels like solving a layered puzzle. Symptoms are subtle, presentations are atypical, and medical conditions frequently overlap with psychiatric ones. In this context, standardized assessment instruments are not optional—they are essential.
They bring structure to complexity, help clinicians move beyond subjective impressions, and allow tracking of illness over time. More importantly, they help us answer the most important question in geriatric care:
👉 “How is this person functioning in real life?”
Why Do We Need Assessment Tools in the Elderly?
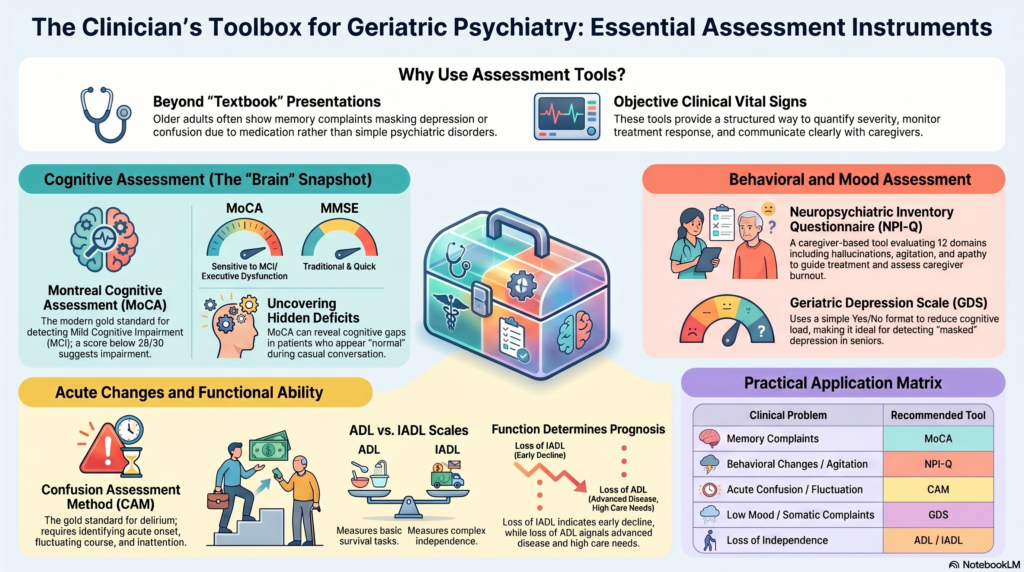
Older adults rarely present with “textbook psychiatry.”
Instead, we see:
- Memory complaints masking depression
- Agitation caused by infection or pain
- Confusion due to medications
- Behavioral changes in dementia
Clinical interviews alone can miss early or subtle changes. Assessment tools help us:
- Screen for disorders early
- Differentiate between conditions (e.g., delirium vs dementia)
- Quantify severity
- Monitor progression and response to treatment
- Communicate objectively with caregivers and teams
👉 In simple terms:
Assessment tools are the “vital signs” of geriatric mental health.
Core Domains of Assessment
A good geriatric psychiatric evaluation is not limited to diagnosis. It spans multiple domains:
- Cognition – memory, attention, executive function
- Behavior – agitation, psychosis, sleep changes
- Mood – depression, anxiety
- Function – independence in daily living
- Acute changes – delirium
Each domain has specific tools that enhance clinical clarity.
1. Cognitive Assessment Tools
Montreal Cognitive Assessment (MoCA)
The MoCA has emerged as one of the most useful screening tools in modern geriatric psychiatry.
What it assesses:
- Attention and concentration
- Executive function
- Memory
- Language
- Visuospatial ability
- Orientation
Scoring:
- Total score: 30
- ≥26 = Normal
- <26 suggests cognitive impairment
Why MoCA matters:
- Detects Mild Cognitive Impairment (MCI)
- More sensitive than traditional tools like MMSE
- Picks up early dementia
👉 Clinical insight:
If a patient complains of “forgetfulness” but appears normal on casual conversation, MoCA often reveals the hidden deficit.
Mini-Mental State Examination (MMSE)
The MMSE is the traditional cognitive screening tool.
Strengths:
- Quick and widely known
- Useful in moderate to severe dementia
Limitations:
- Less sensitive for early cognitive decline
- Misses executive dysfunction
👉 Today, MMSE is often supplemented or replaced by MoCA in early screening.
2. Behavioral Assessment
Neuropsychiatric Inventory Questionnaire (NPI-Q)
Dementia is not just about memory—it is about behavior.
The NPI-Q is a caregiver-based instrument designed to assess Behavioral and Psychological Symptoms of Dementia (BPSD).
It evaluates 12 domains:
- Delusions
- Hallucinations
- Agitation/aggression
- Depression
- Anxiety
- Apathy
- Irritability
- Disinhibition
- Sleep disturbances
- Appetite changes
What it measures:
- Presence of symptoms
- Severity (mild to severe)
- Caregiver distress
Why it is crucial:
- Behavioral symptoms are the main reason for caregiver burnout
- They often determine hospitalization or institutionalization
- They guide treatment decisions (non-pharmacological vs pharmacological)
👉 Clinical insight:
Two patients with the same cognitive score may behave very differently.
MoCA tells you cognition—NPI-Q tells you real-world impact.
3. Delirium Assessment
Confusion Assessment Method (CAM)
Delirium is one of the most common and most missed conditions in the elderly.
The CAM is the gold standard screening tool.
Diagnosis requires:
- Acute onset + fluctuating course
- Inattention
AND - Disorganized thinking OR altered consciousness
Why CAM matters:
- Delirium is often reversible
- Missing it can lead to serious outcomes
- Helps differentiate from dementia
👉 Clinical insight:
If cognition fluctuates during the day → think delirium → use CAM.
4. Depression Assessment
Geriatric Depression Scale (GDS)
Depression in older adults often presents differently:
- More somatic symptoms
- Less verbalized sadness
- Overlap with cognitive complaints
The GDS simplifies assessment.
Features:
- Yes/No format
- Easy to administer
- Minimal cognitive load
Why it is useful:
- Ideal for elderly patients
- Helps detect masked depression
5. Functional Assessment
ADL and IADL Scales
In geriatrics, diagnosis alone is not enough.
Function determines prognosis.
ADL (Basic Activities):
- Bathing
- Dressing
- Eating
- Toileting
IADL (Complex Activities):
- Managing money
- Taking medications
- Cooking
- Transport
Why they matter:
- Predict independence and survival
- Help in care planning
- Distinguish severity of dementia
👉 Clinical insight:
Loss of IADL = early decline
Loss of ADL = advanced disease
6. Other Useful Tools (Quick Overview)
- Clinical Dementia Rating (CDR) → severity staging
- Richmond Agitation Sedation Scale (RASS) → agitation level
- Delirium Rating Scale (DRS) → severity of delirium
- Frailty Index → biological vulnerability
Putting It All Together: A Practical Approach
A structured approach can simplify clinical work:
| Clinical Problem | Tool |
|---|---|
| Memory complaint | MoCA |
| Behavioral changes | NPI-Q |
| Acute confusion | CAM |
| Low mood | GDS |
| Loss of independence | ADL / IADL |
The Bigger Picture
Assessment instruments do not replace clinical judgment—they refine it.
They help us:
- Detect problems early
- Avoid misdiagnosis
- Reduce unnecessary medication
- Support caregivers
- Improve outcomes
Final Reflection
Geriatric psychiatry is not just about diagnosing disorders—it is about understanding how a person lives, thinks, and behaves in their real world.
👉 MoCA shows how the brain works.
👉 NPI-Q shows how the illness affects life.
Together, they transform clinical care from guesswork to precision.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808