Aging vs Dementia: How to Identify Neurocognitive Dysfunction Early
 Aging Is Not Dementia
Aging Is Not Dementia
Forgetfulness in older adults is common, but it is not always dementia. The clinical challenge is to distinguish normal cognitive aging, subjective cognitive decline, mild cognitive impairment, major neurocognitive disorder, delirium, and depression-related cognitive dysfunction.
The World Health Organization gives a simple public-health definition: “Dementia is a term for several diseases” affecting memory, thinking and daily activities. WHO also notes that dementia is not an inevitable consequence of aging and that mood, behaviour and motivation changes may accompany or even precede cognitive impairment.
For families, the practical question is not merely:
“Does the person forget?”
The more important clinical question is:
“Is there a progressive decline from the person’s previous level, and is it affecting independence, judgment, behaviour or daily functioning?”
The Scientific Continuum: From Aging to Dementia
Cognitive symptoms in older adults can be understood as a spectrum.
1. Normal Cognitive Aging
Normal aging may involve slower processing speed, occasional word-finding difficulty, reduced multitasking efficiency, and slower retrieval of names or details. However, independence is preserved. The person can still manage medicines, money, cooking, travel, hygiene, phone use and social judgment.
In normal aging, memory lapses are usually occasional, non-progressive, and improved by cues or reminders.
2. Subjective Cognitive Decline
In subjective cognitive decline, the person feels that memory or thinking has worsened, but objective testing may be normal. This is clinically important because it may reflect anxiety, depression, poor sleep, stress, early neurodegeneration, or increased self-monitoring.
A person may say, “I am forgetting more than before,” but still function normally. This group needs observation, risk-factor assessment, and follow-up rather than immediate labelling.
3. Mild Cognitive Impairment / Mild Neurocognitive Disorder
Mild cognitive impairment is more than normal aging but not yet dementia. The Alzheimer’s Association describes MCI as cognitive change that is serious enough to be noticed but does not significantly affect everyday activities.
DSM-5-TR uses the term mild neurocognitive disorder. The essential idea is:
- There is modest cognitive decline from a previous level.
- Decline is noticed by the patient, informant, or clinician.
- Objective testing supports impairment.
- Independence is largely preserved, though the person may need more effort, reminders or compensatory strategies.
- It is not better explained by delirium or another mental disorder.
4. Dementia / Major Neurocognitive Disorder
Dementia, or major neurocognitive disorder, implies cognitive decline severe enough to impair independent functioning.
The NIA-AA all-cause dementia criteria include the key functional threshold: “Interfere with the ability to function at work or at usual activities.”
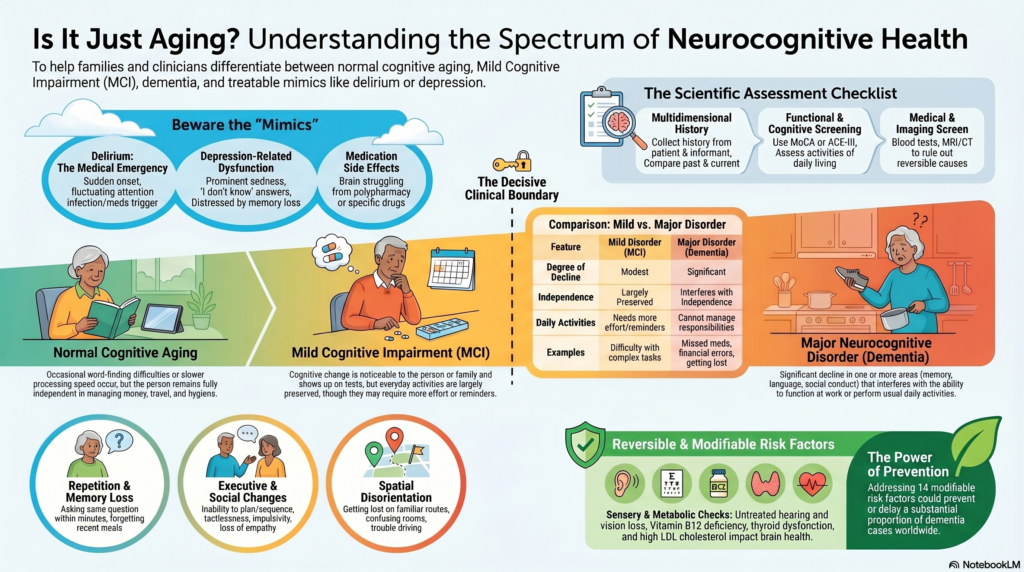
This is the decisive clinical boundary. Forgetting names is not enough. Dementia is suspected when cognitive or behavioural decline disrupts daily life: medicines, finances, cooking, safety, social conduct, judgment, route-finding or self-care.
DSM-5-TR Style Clinical Criteria: Mild vs Major Neurocognitive Disorder
A scientific way to frame the distinction is:
| Domain | Mild Neurocognitive Disorder / MCI | Major Neurocognitive Disorder / Dementia |
|---|---|---|
| Degree of decline | Modest decline | Significant decline |
| Cognitive domains | One or more domains | One or more domains |
| Functional independence | Largely preserved | Interferes with independence |
| Daily activities | More effort, reminders or compensation needed | Patient cannot reliably manage previous responsibilities |
| Examples | Repeated reminders, difficulty with complex tasks | Missed medicines, financial errors, unsafe cooking, getting lost |
| Exclusions | Not delirium, not better explained by depression or another disorder | Not delirium, not better explained by another psychiatric/medical cause |
DSM-5-TR cognitive domains include complex attention, executive function, learning and memory, language, perceptual-motor function and social cognition. This matters because dementia is not always first seen as memory loss. In frontotemporal dementia, early symptoms may be disinhibition, apathy, loss of empathy or compulsive behaviour. In Lewy body dementia, visual hallucinations, fluctuations and REM sleep behaviour symptoms may be prominent.
ICD-11 Perspective: Neurocognitive Disorders
ICD-11 places dementia within neurocognitive disorders, emphasizing decline in cognitive functioning acquired after a period of normal development. ICD-11 also recognises mild neurocognitive disorder, which is characterized by mild impairment in one or more cognitive domains relative to what is expected for age.
This is clinically useful because it avoids the simplistic binary of “normal” versus “dementia.” Many older adults fall into an intermediate zone where early identification, monitoring and risk-factor correction are valuable.
NICE Guideline Approach: Diagnosis Should Not Depend on One Memory Test
NICE NG97 recommends that initial dementia assessment should include cognitive, behavioural and psychological symptoms, functional impact, history from the patient, and if possible, history from someone who knows the person well. It also recommends physical examination, blood and urine tests to exclude reversible causes, and cognitive testing.
One important NICE warning is worth quoting: “Do not rule out dementia solely because the person has a normal score.”
This is highly relevant in Indian clinical practice. A highly educated person may score normally in early disease. A person with low literacy may score poorly without dementia. Hearing impairment, visual impairment, language, depression, anxiety, fatigue and cultural factors can all distort cognitive test scores.
Therefore, a memory clinic assessment should combine:
- Patient history
- Informant history
- Functional assessment
- Cognitive screening
- Mood and sleep evaluation
- Medication review
- Neurological and medical assessment
- Relevant blood tests
- Imaging when clinically indicated
Better Clinical Red Flags Than “Memory Loss”
The following features are more predictive of neurocognitive disorder than occasional forgetfulness:
Functional decline
The person now struggles with medicines, money, bills, cooking, phone use, travel, hygiene or appointments.
Repetition
They ask the same question repeatedly within minutes or hours.
Loss of recent memory
They forget recent conversations, meals, visits or events, while older memories remain relatively preserved.
Executive dysfunction
They cannot plan, sequence, solve problems or handle previously familiar tasks.
Social cognition change
There is new tactlessness, poor judgment, reduced empathy, impulsivity or socially inappropriate behaviour.
Spatial disorientation
They get lost in familiar routes, confuse rooms, misjudge distances or have trouble parking/driving.
Behavioural symptoms
Suspiciousness, apathy, irritability, aggression, wandering, sleep reversal, hallucinations or refusal of care may appear.
WHO explicitly lists early symptoms such as forgetting recent events, losing things, getting lost, confusion in familiar places, losing track of time, difficulty solving problems and trouble finding words.
Depression vs Dementia: The Pseudodementia Problem
Depression in late life can mimic dementia. Patients may show poor concentration, slowed thinking, low motivation, poor sleep, appetite change, fatigue and memory complaints.
However, the distinction is not always clean. Depression can mimic dementia, dementia can cause depression, and both can coexist.
Clinical clues suggesting depression-related cognitive dysfunction include prominent sadness, guilt, hopelessness, early morning worsening, loss of interest, sleep/appetite disturbance, and repeated “I don’t know” answers. Patients with depression may be very distressed by their memory symptoms.
Clinical clues suggesting dementia include progressive functional decline, poor insight, repeated questions, getting lost, impaired instrumental activities of daily living, and informant-reported change.
A useful principle: do not diagnose dementia without assessing depression, and do not diagnose depression without assessing cognition in an older adult.
Delirium vs Dementia: The Emergency Distinction
Delirium is an acute medical brain syndrome. It is often missed in elderly patients and may be mistaken for dementia.
NICE delirium guidance advises clinicians to look for recent changes or fluctuations occurring within hours or days, especially in older adults, those with cognitive impairment, hip fracture or severe illness.
A practical distinction:
| Feature | Dementia | Delirium |
|---|---|---|
| Onset | Gradual | Sudden |
| Time course | Months to years | Hours to days |
| Fluctuation | Less marked early | Marked fluctuation |
| Attention | Relatively preserved early | Prominently impaired |
| Consciousness | Usually clear until later | Altered alertness common |
| Cause | Neurodegenerative/vascular/mixed | Infection, dehydration, drugs, metabolic illness, surgery, pain |
| Urgency | Needs evaluation | Medical urgency |
NICE dementia guidance is very clear: if it is not possible to distinguish delirium from dementia or delirium superimposed on dementia, treat for delirium first.
For families, the rule is simple:
Gradual decline suggests dementia. Sudden confusion is delirium until proven otherwise.
Medication-Induced Cognitive Impairment
Medication review is central in geriatric psychiatry. NICE recommends referral to specialist dementia diagnostic services only after reversible causes have been investigated, including delirium, depression, sensory impairment and medicines associated with increased anticholinergic burden.
Common medication contributors include:
- Benzodiazepines and Z-drugs
- Sedating antihistamines
- Anticholinergic bladder medicines
- Tricyclic antidepressants
- Opioids and centrally acting pain medicines
- Polypharmacy
- High sedative load
- Incorrect dosing in renal/hepatic impairment
In older adults, the clinical question is often not “Which tablet should we add?” but “Which tablet is the brain struggling to tolerate?”
Reversible and Modifiable Causes to Check
A structured evaluation should look for:
- Depression and anxiety
- Delirium
- Sleep apnea and chronic insomnia
- Vitamin B12 deficiency
- Thyroid dysfunction
- Anemia
- Electrolyte disturbance, especially sodium
- Diabetes and hypoglycemia
- Hypertension and vascular risk
- Hearing impairment
- Visual impairment
- Alcohol use
- Medication adverse effects
- Stroke, Parkinson’s disease or head injury
- Social isolation and cognitive inactivity
The 2024 Lancet Commission added two newer modifiable risk factors—high LDL cholesterol and untreated vision loss—and estimated that addressing 14 modifiable risk factors could prevent or delay a substantial proportion of dementia cases.
This is important for India, where vascular risk, diabetes, hypertension, sensory impairment and social isolation often overlap with cognitive decline.
What a Scientific Memory Clinic Assessment Should Include
A proper assessment should not be limited to MMSE or MoCA alone.
1. History of cognitive decline
Onset, progression, domains affected, speed of worsening, and comparison with previous functioning.
2. Informant history
Family observations are crucial because insight may be impaired in dementia.
3. Functional assessment
Activities of daily living and instrumental activities of daily living: medicines, finances, cooking, travel, phone use, shopping, hygiene, safety.
4. Cognitive testing
MoCA, MMSE, ACE-III, Mini-Cog, 6-CIT, GPCOG, FAQ, IQCODE or other tools depending on education, language and clinical context.
5. Psychiatric assessment
Depression, anxiety, psychosis, apathy, sleep disturbance, irritability, personality change, suicidal ideation and caregiver stress.
6. Medication review
Anticholinergic burden, sedative load, polypharmacy, drug interactions and inappropriate long-term hypnotic use.
7. Medical and neurological screen
Stroke, Parkinsonism, gait, falls, seizures, head injury, sensory impairment, metabolic illness.
8. Investigations
CBC, electrolytes, renal/liver function, thyroid profile, vitamin B12, folate when relevant, glucose/HbA1c and other tests based on clinical context.
9. Imaging
NICE recommends structural imaging to rule out reversible causes and assist subtype diagnosis unless dementia is already well established and subtype is clear.
Where Biomarkers Fit: Scientific but Not Always First-Line
Modern Alzheimer’s diagnosis is moving toward biological markers. The 2024 Alzheimer’s Association criteria state that Alzheimer’s disease should be defined biologically and diagnosed by core biomarker abnormalities, but they also clarify that these criteria are not step-by-step clinical workflow guidelines.
For routine clinical practice in India, biomarkers such as amyloid PET, tau PET, CSF biomarkers and plasma biomarkers may be useful in selected cases, but they are not required for every elderly person with memory complaints. Cost, availability, pre-test probability, treatment implications and family counselling matter.
The practical sequence remains:
Clinical syndrome → functional impact → exclusion of reversible causes → subtype assessment → selective biomarkers/imaging when they will change management.
Why Early Diagnosis Matters
Early diagnosis matters because it allows:
- Treatment of reversible contributors
- Correction of depression, sleep and anxiety
- Medication simplification
- Vascular risk reduction
- Cognitive stimulation and activity planning
- Caregiver education
- Home safety planning
- Advance care and legal planning
- Prevention of crisis-driven decisions
- Reduction of blame within families
The AAN guideline on MCI found no high-quality evidence for pharmacological treatment of MCI, but states: “Clinicians should recommend regular exercise.” It also notes that cognitive training may improve cognitive measures.
This is a powerful message for families: early cognitive symptoms do not always mean starting dementia medicines. Often the first intervention is scientific lifestyle correction, risk-factor control, sleep improvement, mood treatment and follow-up.
A Practical Clinical Threshold for Families
Seek assessment when any of the following occur:
- Repeated questioning
- Forgetting recent events
- Getting lost in familiar places
- Missing medicines
- Financial mistakes
- Unsafe cooking
- New suspiciousness
- Personality change
- Poor judgment
- Sleep reversal
- Hallucinations
- Wandering
- Decline in hygiene
- Depression with memory complaints
- Sudden confusion
- Caregiver burnout
Urgent medical review is needed if confusion is sudden, fluctuating, associated with fever, drowsiness, dehydration, falls, weakness, seizures, head injury or reduced consciousness.
Conclusion
Normal aging slows cognition. Mild cognitive impairment causes measurable decline but largely preserves independence. Dementia causes progressive cognitive or behavioural decline that interferes with daily life. Delirium is sudden and medically urgent. Depression, poor sleep, sensory impairment and medications can mimic or worsen cognitive dysfunction.
The scientific approach is not to label every older adult with forgetfulness as dementia. It is also not to dismiss progressive decline as “just aging.”
The correct approach is structured, guideline-informed assessment.
Memory care is not only about memory. It is about brain function, mood, behaviour, sleep, safety, dignity, caregiver survival and early planning.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
Dr. Srinivas Rajkumar T provides structured assessment and treatment for memory loss, neurocognitive dysfunction, dementia-related behavioural symptoms, depression, anxiety, sleep problems and caregiver stress in older adults.
Related posts:
- Aging vs Dementia: Understanding Neurocognitive Dysfunction
- Teacher’s Guide: How to Identify Learning Disabilities Early in the Classroom
- Autism How parents and caregivers can identify early signs
- Dementia Series: Young-Onset Dementia – When Dementia Strikes Early
- Post-SSRI Sexual Dysfunction in Women: Understanding Frigidity After Antidepressants
- Executive Dysfunction in the Era of Prolonged Digital Consumption