Self-Disorder in Schizophrenia: Ipseity, Development, Corollary Discharge and the Neurophenomenology of Psychosis
 Introduction: Beyond Hallucinations and Delusions
Introduction: Beyond Hallucinations and Delusions
Schizophrenia is often taught through its most visible symptoms: hallucinations, delusions, disorganized speech, negative symptoms and cognitive impairment. Yet these clinical features do not fully capture the deeper transformation that many patients describe. Long before overt psychosis appears, many individuals experience a subtle but profound alteration in the basic sense of existing as a self.
This deeper alteration has been described in phenomenological psychiatry as the “core Gestalt” of schizophrenia. It refers not merely to a collection of symptoms, but to a characteristic transformation in the structure of subjectivity itself. The patient’s relation to self, body, thought, action, other people and the world becomes altered.
The concept of Self-Disorder, or anomalous self-experience, attempts to describe this transformation. It is not simply low self-esteem, identity confusion, dissociation or personality disturbance. Rather, it refers to disruption in the most basic, prereflective sense that “I am the subject of my experiences.”
In ordinary life, we do not usually notice this basic selfhood. Thoughts, perceptions, movements and emotions are immediately experienced as “mine.” In schizophrenia-spectrum conditions, this implicit self-presence may become unstable. Thoughts may feel object-like. The body may feel strange or distant. The world may appear artificial, excessively meaningful or subtly unreal. Social life may become difficult not only because of anxiety or suspiciousness, but because the basic anchoring of self in the shared world is weakened.
This is why self-disorders are increasingly regarded as a crucial phenotype for understanding schizophrenia-spectrum vulnerability.
Minimal Self and Reflective Self
A useful distinction is between the Minimal Self and the Reflective Self.
The Minimal Self is the immediate, first-person quality of experience. It is the silent sense that my thoughts, actions and perceptions belong to me. It is not a belief about oneself, but the structure through which experience is lived.
The Reflective Self is the self that can think about itself. It includes autobiography, identity, values, roles, memories and social self-understanding.
In schizophrenia-spectrum vulnerability, the disturbance appears to begin at the level of the Minimal Self. Later, as development progresses, the Reflective Self becomes increasingly aware of these subtle anomalies. This may explain why many self-disorders become more clinically visible in late childhood and adolescence, even if their roots may lie much earlier in development.
The Ipseity-Disturbance Model
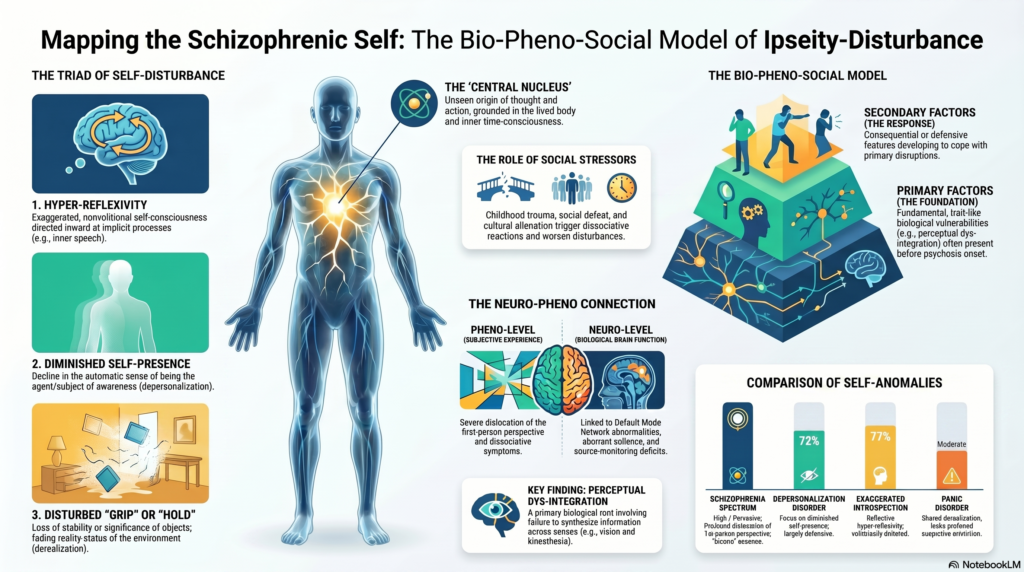
The Ipseity-Disturbance Model, associated especially with Sass and Parnas, proposes that schizophrenia involves a disturbance of ipseity: the basic sense of selfhood or first-person givenness.
The model has three central components.
First, there is diminished self-presence. The person may feel less naturally present in their own experience. They may describe feeling empty, unreal, ghost-like, detached or not fully existing.
Second, there is hyperreflexivity. Normally automatic processes become objects of excessive awareness. A person may begin noticing their own thoughts, bodily sensations, intentions or perceptions in a strange, objectified way. The mind turns back upon itself.
Third, there is disturbed grip on the world. The ordinary sense of being smoothly immersed in reality weakens. The world may feel uncanny, artificial, staged, distant or over-significant.
These three processes interact. As self-presence weakens, the person may become more hyperreflective. As hyperreflexivity increases, spontaneous immersion in the world becomes further disrupted. This can create the experiential soil from which delusions, hallucinations and passivity phenomena later emerge.
Clinical Phenomenology of Self-Disorder
Self-disorders may appear clinically as:
- Disturbed stream of consciousness
Thoughts may feel fragmented, spatialized, pressured, blocked or externally accessible. - Disturbed self-presence
The person may feel they are observing themselves from a distance, or that their inner life lacks natural vitality. - Disturbed bodily experience
The body may feel mechanical, alien, disproportionate, unreal or detached. - Disturbed self-world boundary
The person may feel excessively open to others, invaded by the world, or uncertain where self ends and the world begins. - Existential reorientation
The person may become preoccupied with metaphysical, solipsistic or cosmic questions in a way that is not merely philosophical but experientially urgent. - Hyperreflexivity
Ordinary acts such as thinking, speaking, walking or looking at others may become objects of painful self-monitoring.
These experiences may remain non-psychotic for years. However, they can later crystallize into psychotic symptoms. For example, a vague feeling that one’s thoughts are not fully one’s own may later become thought insertion. A disturbed sense of bodily agency may later become delusions of control. An uncanny sense that the world is arranged around oneself may later become delusions of reference.
EASE and the Measurement of Self-Disorder
The Examination of Anomalous Self-Experience, or EASE, was developed to systematically assess these subtle phenomena. This was a major advance because it transformed self-disorder from a purely descriptive concept into a clinically measurable research phenotype.
The EASE explores domains such as cognition and stream of consciousness, self-awareness and presence, bodily experience, demarcation between self and world, and existential reorientation.
Research using EASE has shown that self-disorders aggregate strongly in schizophrenia-spectrum conditions compared with other psychiatric disorders and healthy controls. They also appear in schizotypal and high-risk populations, suggesting that they may index vulnerability before overt psychosis emerges.
Clinical Utility
Self-disorder has four major clinical uses.
First, it improves early identification. Adolescents who present with social withdrawal, anxiety, oddness, existential perplexity or attenuated psychotic symptoms may be better understood if clinicians assess for disturbances in basic selfhood.
Second, it has prognostic value. Persistent self-disorders may indicate higher risk for schizophrenia-spectrum progression, especially when combined with functional decline, negative symptoms, family history or attenuated psychotic symptoms.
Third, it improves diagnostic precision. A patient with unusual beliefs may be psychotic, obsessive, autistic, traumatized or personality-disordered. Assessment of self-disorder helps clarify whether the underlying structure of experience resembles schizophrenia-spectrum psychopathology.
Fourth, it supports research. Self-disorder may function as a trait phenotype for genetic, developmental and neurobiological studies. It may also offer new psychotherapeutic targets, especially around embodiment, agency, intersubjectivity and world-immersion.
Feyaerts and Sass: Revising the Ipseity Model
Recent work by Feyaerts and Sass has challenged and refined the classical Ipseity-Disturbance Model.
Their critique has three main parts.
First, they question whether self-disorders are entirely specific to schizophrenia. Similar-looking phenomena may occur in trauma, dissociation, autism, borderline personality disorder and severe affective illness.
Second, they argue that self-disorder cannot be understood as an isolated intrapsychic phenomenon. Selfhood is always relational and embedded in interpersonal life.
Third, they point out that finding specific neural correlates of self-disorder remains difficult.
Their revision emphasizes that self-presence and grip on the world should not be understood only as diminished. They may also become intensified or distorted. For example, a person may feel not only detached from the world, but also strangely central to it. They may experience themselves as cosmically significant, watched, transparent or ontologically exposed.
They also place greater emphasis on hyperreflexivity. Hyperreflexivity is not merely excessive thinking. It is a shift in the structure of consciousness where normally tacit processes become explicit, alien and object-like.
This revision enriches the model by making it more dynamic. However, a purely structural model remains incomplete unless it explains how these disturbances arise developmentally.
The Developmental Turn: Ontogenesis of Self-Disorder
The 2025 Raballo, Henriksen, Poletti and Parnas paper argues that self-disorder must be understood developmentally. The key question is not only “What is disturbed?” but “How does this disturbance emerge across development?”
The authors challenge the assumption that the self is fully intact before illness onset. Instead, they suggest that subtle alterations of Minimal Selfhood may be present early, while reflective awareness of these alterations becomes clearer later.
In childhood, the self develops through bodily action, sensorimotor integration, attachment, language, mirroring, play and social participation. A child gradually learns not only “this is my body” and “this is my action,” but also “I am a stable subject in a shared world.”
If this developmental process is subtly altered, the child may grow with an unstable sense of agency, embodiment and intersubjective anchoring. By adolescence, when self-reflection becomes more sophisticated, these implicit disturbances may become thematically available. The adolescent may begin to ask: “Why do I feel unreal?” “Why do my thoughts feel strange?” “Why do others seem to know what I am thinking?” “Why does the world feel staged?”
Thus, adolescence may not be the beginning of self-disorder. It may be the period when the Reflective Self becomes able to recognize and suffer from earlier disturbances in the Minimal Self.
Environmental Perturbations and Selfhood
Selfhood is not built in isolation. Early adversity, chronic invalidation, emotional neglect, intrusive parenting, trauma and disrupted attachment may influence the developing sense of agency and self-coherence.
This does not mean that poor parenting causes schizophrenia. Rather, environmental perturbations may interact with genetic and neurodevelopmental vulnerability.
A child who repeatedly experiences the world as unpredictable, intrusive or poorly attuned may develop weaker confidence in their own perceptions, intentions and agency. In a biologically vulnerable individual, such disruptions may contribute to later instability in self-experience.
This developmental view helps bridge phenomenology with social psychiatry. Self-disorder is not simply “inside the brain” and not simply “caused by society.” It emerges through brain-body-world development.
Corollary Discharge as a Neurobiological Bridge
Corollary discharge provides one of the most promising neurophysiological bridges between self-disorder and brain function.
When the brain initiates an action, it generates an internal copy of that motor command. This efference copy predicts the sensory consequences of the action. If the predicted and actual sensations match, the brain recognizes the event as self-generated.
This mechanism explains why one’s own voice, movement or touch feels self-produced. It also explains why self-generated sensations are usually attenuated compared with externally generated sensations.
In schizophrenia, corollary discharge mechanisms appear impaired. This may weaken the distinction between self-generated and externally generated experiences.
Clinically, this can help explain:
- auditory hallucinations,
- thought insertion,
- passivity phenomena,
- delusions of control,
- disturbed agency,
- alienation of inner speech.
If inner speech is not properly tagged as self-generated, it may be experienced as coming from outside. If actions are not predicted as self-generated, they may feel externally controlled. If thoughts lack the usual sense of ownership, they may feel inserted, broadcast or shared.
Recent electrophysiological work has begun linking impaired corollary discharge with anomalous self-experiences, giving the self-disorder model a more measurable neurophysiological substrate.
Predictive Processing and Self-Disorder
Predictive processing extends the corollary discharge model. The brain is not a passive receiver of information; it actively predicts sensory input and updates its model of the world based on prediction errors.
Selfhood itself may depend on stable prediction. I experience my body as mine because my brain can predict the sensory consequences of my movements. I experience my thoughts as mine because they arise within a stable model of agency and ownership. I experience the world as real because prediction and sensory evidence are sufficiently integrated.
In schizophrenia, prediction errors may become abnormally weighted. The brain may assign excessive importance to noise, fail to attenuate self-generated stimuli, and struggle to stabilize high-level beliefs.
This framework links several models:
- corollary discharge failure,
- aberrant salience,
- dysconnection,
- NMDA hypofunction,
- Bayesian inference abnormalities,
- ipseity disturbance.
In this integrated view, self-disorder is not merely a philosophical concept. It may reflect instability in the predictive architecture that normally sustains embodied selfhood.
Aberrant Salience and Self-Disorder
Aberrant salience explains why neutral events become charged with excessive significance. Dopaminergic dysregulation may cause ordinary stimuli to feel unusually important, threatening or personally meaningful.
Self-disorder may provide the vulnerable experiential background upon which aberrant salience acts.
For example, if a person already feels unstable in their self-world boundary, a neutral glance from another person may not simply feel noticeable; it may feel personally directed. If the world already feels uncanny, a random event may become evidence of hidden meaning. If thoughts already feel alien, a coincidental external sound may seem connected to one’s mind.
Thus, aberrant salience may help explain the motivational and affective force of delusion formation, while self-disorder explains why the person’s basic relation to self and world is already vulnerable.
Dysconnection and NMDA Hypofunction
The dysconnection hypothesis proposes that schizophrenia involves abnormal integration between brain regions rather than dysfunction of a single area. NMDA receptor hypofunction is often proposed as a mechanism that may disturb synaptic plasticity, cortical coordination and hierarchical prediction.
From a self-disorder perspective, dysconnection may disrupt the integration of sensorimotor, interoceptive, social and cognitive signals required for stable selfhood.
The self is not located in one brain region. It emerges from coordinated processes involving body signals, motor prediction, memory, emotion, perception, social cognition and language. Dysconnection may therefore destabilize the very integration that allows experience to feel unified and mine.
Self-Disorder Across the Schizophrenia Spectrum
Self-disorders are relevant not only in established schizophrenia but across the broader schizophrenia spectrum.
They may appear in:
- schizotypal personality structures,
- familial high-risk states,
- clinical high-risk for psychosis,
- early-onset schizophrenia,
- first-episode psychosis,
- chronic schizophrenia.
Their presence in non-psychotic high-risk states is especially important. It suggests that self-disorder is not simply a consequence of hallucinations or delusions. Rather, it may precede and shape them.
Differential Diagnosis
A major clinical challenge is distinguishing self-disorder from superficially similar phenomena.
In dissociation, the person may feel detached from self or body, often in relation to trauma and affective overwhelm. In autism, differences in social cognition, sensory processing and embodiment may produce unusual self-world relations, but not necessarily the same ipseity disturbance. In borderline personality disorder, identity instability is often interpersonal, affective and autobiographical rather than primarily prereflective. In OCD, intrusive thoughts are ego-dystonic but usually recognized as one’s own. In depersonalization disorder, unreality is prominent but reality testing is usually preserved.
In schizophrenia-spectrum self-disorder, the disturbance is often more basic: the very first-person structure of experience is altered. The person may not merely say, “I feel detached,” but “my thoughts do not arise as mine,” “my body is not properly inhabited,” or “the world and I no longer fit together naturally.”
Implications for Psychotherapy
If self-disorder is central to schizophrenia, psychotherapy should not focus only on correcting delusional beliefs. It should also help the person regain a more stable, embodied and interpersonal sense of self.
Potential therapeutic targets include:
- strengthening bodily grounding,
- improving agency through structured action,
- reducing maladaptive hyperreflexivity,
- supporting narrative coherence,
- restoring interpersonal trust,
- helping patients describe anomalous experiences without immediate delusional elaboration,
- building shared reality through collaborative reflection.
A phenomenologically informed therapy does not dismiss unusual experiences. It helps the patient articulate them safely, link them to stress and development, and reduce their frightening opacity.
Research Directions
Future research should integrate four levels.
First, phenomenology: careful first-person description of anomalous self-experience.
Second, development: longitudinal study of children and adolescents at risk.
Third, neurophysiology: measures such as corollary discharge, sensory attenuation, EEG markers, oculomotor prediction and speech-related N1 suppression.
Fourth, computational modeling: predictive processing, precision weighting, active inference and hierarchical Bayesian models.
The most promising future model will not be purely phenomenological or purely biological. It will be neurophenomenological and developmental.
Conclusion
Self-disorder may be one of the most important concepts for understanding schizophrenia beyond its surface symptoms. It captures the subtle, trait-like transformation of subjectivity that often precedes psychosis and shapes later symptom formation.
The Ipseity-Disturbance Model remains a powerful framework, but recent revisions show the need to understand self-disorder dynamically, interpersonally and developmentally. The 2025 developmental account adds an important corrective: self-disorder should not be viewed as a timeless structural abnormality, but as a trajectory unfolding across childhood, adolescence and illness progression.
Corollary discharge provides a crucial neurobiological bridge. By linking impaired self-monitoring with disturbances of agency and ownership, it allows phenomenological psychiatry to converse with cognitive neuroscience.
Ultimately, schizophrenia may be best understood not simply as a disorder of dopamine, hallucinations or delusions, but as a disorder of the developing self: a condition in which the most basic sense of being an embodied subject in a shared world becomes unstable, fragile and painfully exposed.