Thomas and Chess Temperament Theory: A Scientific Framework for Understanding Child Behaviour
 Introduction
Introduction
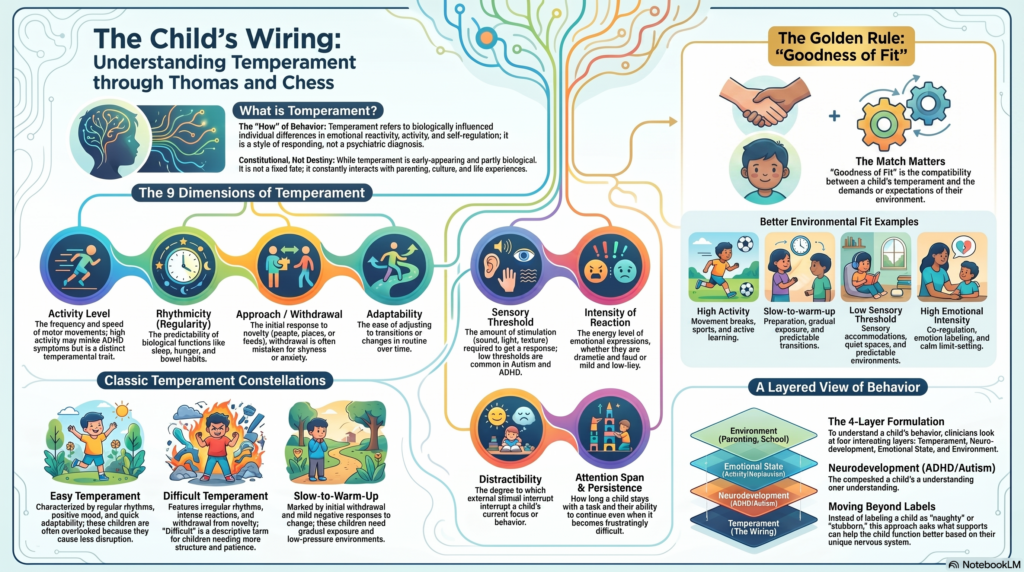
Temperament refers to biologically influenced, early-appearing individual differences in emotional reactivity, motor activity, attention, adaptability, and self-regulation.
It is not the same as personality, behaviour, discipline, or psychiatric diagnosis. Temperament describes the child’s style of responding to internal and external stimuli.
For example, two children may both refuse school. One may be anxious, another may have autism-related sensory overload, another may have ADHD-related executive dysfunction, and another may simply be slow to adapt to new environments. The visible behaviour may be similar, but the temperamental and clinical formulation may differ.
The work of Alexander Thomas and Stella Chess, particularly through the New York Longitudinal Study, provided one of the earliest systematic models of childhood temperament. Their work was important because it shifted child psychiatry away from simplistic parent-blaming models and toward a more transactional understanding: the child’s temperament and the environment continuously influence each other.
Temperament: Definition
Temperament may be defined as the child’s characteristic pattern of:
- emotional reactivity,
- activity level,
- biological regularity,
- response to novelty,
- sensory sensitivity,
- adaptability,
- attention,
- persistence,
- and mood quality.
Temperament is partly constitutional, but not fixed destiny. It interacts with parenting, family stress, school demands, culture, sleep, neurodevelopment, trauma, and psychiatric vulnerability.
Thomas and Chess: The Nine Temperament Dimensions
| No. | Temperament Dimension | Scientific Meaning | High-End Presentation | Low-End Presentation | Clinical Relevance |
|---|---|---|---|---|---|
| 1 | Activity Level | Overall level of motor activity and bodily movement | Constant movement, climbing, running, difficulty sitting still | Calm, less physically active, prefers quiet activity | High activity may mimic or amplify ADHD symptoms, but activity level alone is not ADHD |
| 2 | Rhythmicity / Regularity | Predictability of biological functions such as sleep, hunger, bowel habits, and routines | Predictable sleep, feeding, waking, toileting patterns | Irregular sleep, appetite, energy, daily rhythm | Irregularity may increase parenting stress and worsen sleep or routine-related behavioural problems |
| 3 | Approach / Withdrawal | Initial response to new people, places, foods, activities, or situations | Moves toward novelty, explores easily, socially open | Hesitates, clings, cries, avoids, observes first | Withdrawal may be mistaken for anxiety, autism, shyness, or oppositionality |
| 4 | Adaptability | Ease of adjustment after initial exposure to change | Adjusts quickly after initial discomfort | Takes long to adjust; resists transitions and change | Low adaptability is relevant in anxiety, autism spectrum traits, school refusal, and transition difficulties |
| 5 | Sensory Threshold | Amount of stimulation required to produce a response | High threshold: needs stronger stimulation, may seek sensory input | Low threshold: easily disturbed by sound, light, texture, smell, touch | Low threshold is clinically important in autism, ADHD, anxiety, sensory processing difficulties |
| 6 | Intensity of Reaction | Energy level of emotional response | Loud crying, strong anger, dramatic distress, intense excitement | Mild emotional expression, low-intensity reactions | High intensity increases risk of being labelled “dramatic,” “stubborn,” or “manipulative” |
| 7 | Quality of Mood | Predominant emotional tone across situations | Generally cheerful, positive, pleasant | Frequently irritable, serious, negative, dissatisfied | Persistently negative mood requires assessment for depression, anxiety, sleep problems, family stress |
| 8 | Distractibility | Degree to which external stimuli interrupt ongoing behaviour | Easily distracted by sounds, objects, movement, people | Less distractible, stays with current focus | High distractibility may overlap with ADHD but must be interpreted developmentally |
| 9 | Attention Span / Persistence | Duration of attention and ability to continue despite difficulty | Sustains effort, continues despite frustration | Gives up quickly, shifts tasks, poor frustration tolerance | Low persistence may reflect temperament, ADHD, anxiety, learning disorder, depression, or poor executive function |
Classic Temperament Categories
Thomas and Chess described three broad temperament constellations. These are not rigid diagnostic categories. They are descriptive patterns.
| Temperament Pattern | Typical Features | Developmental Meaning | Clinical Caution |
| Easy Temperament | Regular biological rhythms, positive mood, mild to moderate emotional reactions, good adaptability, approach to novelty | Usually adjusts well to routines, school, caregivers, and social expectations | These children may be overlooked because they create less difficulty |
| Difficult Temperament | Irregular rhythms, intense reactions, negative mood, withdrawal from novelty, slow adaptability | Requires more parental patience, structure, predictability, and emotional coaching | “Difficult” is a historical term; it should not be used as a moral label |
| Slow-to-Warm-Up Temperament | Initial withdrawal, mild negative response to novelty, gradual adaptation with repeated exposure | Needs time, preparation, gentle encouragement, and low-pressure exposure | May be mislabelled as shy, anxious, avoidant, rude, or socially uninterested |
Goodness of Fit
The most clinically useful concept from Thomas and Chess is goodness of fit.
Goodness of fit refers to the match between the child’s temperament and the expectations, demands, and responses of the environment.
A temperament is not inherently good or bad. The same trait may become adaptive or maladaptive depending on context.
For example:
| Child Temperament | Poor Environmental Fit | Better Environmental Fit |
| High activity | Long periods of forced sitting, frequent scolding, no movement breaks | Movement breaks, sports, structured activity, active learning |
| Slow-to-warm-up | Forced social performance, criticism for hesitation | Preparation, gradual exposure, predictable transitions |
| Low sensory threshold | Noisy classroom, crowded functions, scratchy clothing, bright lights | Sensory accommodations, quiet spaces, predictable sensory environment |
| High emotional intensity | Adult shouting, punishment during meltdown, shame-based discipline | Co-regulation, emotion labelling, calm limits, repair after conflict |
| Low adaptability | Sudden transitions, unpredictable routine, frequent changes | Visual schedules, warnings before change, rehearsal, transition objects |
The key clinical shift is from asking:
“What is wrong with this child?”
to asking:
“What is the child’s temperament, and how can the environment be adjusted to improve functioning?”
Temperament and Psychopathology
Temperament is not diagnosis, but it can increase vulnerability to certain clinical presentations.
| Temperament Trait | Possible Clinical Association | Important Differential Diagnosis |
| High activity | Hyperactivity, impulsive behaviour, classroom disruption | ADHD, anxiety, sleep deprivation, sensory seeking, trauma |
| High distractibility | Poor academic focus, incomplete tasks | ADHD, learning disorder, anxiety, depression, excessive screen exposure |
| Low adaptability | Meltdowns during change, school refusal, rigid routines | Autism spectrum disorder, anxiety disorder, OCD, adjustment disorder |
| Low sensory threshold | Sensory avoidance, irritability, distress in crowds | Autism, ADHD, anxiety, sensory processing differences |
| High intensity | Tantrums, emotional dysregulation, aggression | ADHD, disruptive behaviour disorder, mood disorder, trauma, family stress |
| Negative mood | Irritability, pessimism, low frustration tolerance | Depression, anxiety, sleep disorder, chronic stress, neurodevelopmental disorder |
| Withdrawal from novelty | Shyness, avoidance, reluctance to try new things | Social anxiety, selective mutism, autism, attachment insecurity |
Temperament should therefore be part of clinical formulation, but it should not be used as a substitute for diagnosis.
Temperament and ADHD
Several temperament dimensions overlap with ADHD-like presentations:
- high activity level,
- high distractibility,
- low persistence,
- poor rhythmicity,
- intense emotional reactions.
However, ADHD requires a persistent, impairing pattern of inattention and/or hyperactivity-impulsivity that is developmentally inappropriate and present across settings.
Temperament can shape the clinical presentation of ADHD. For example, a child with ADHD and high emotional intensity may present with frequent meltdowns, while a child with ADHD and high novelty-seeking may present with risk-taking and rule-breaking.
Temperament and Autism Spectrum Traits
Temperament is also important in autism assessment.
Low adaptability, withdrawal from novelty, sensory sensitivity, intense reactions, and preference for predictability may be seen in some autistic children.
However, autism is not diagnosed from temperament alone. Autism requires assessment of:
- social communication,
- reciprocal social interaction,
- restricted interests,
- repetitive behaviours,
- sensory patterns,
- developmental history,
- and functional impairment.
Temperament may explain part of the child’s behavioural style, but neurodevelopmental assessment is needed when social communication and restricted/repetitive patterns are present.
Temperament and Anxiety
Children who are slow to approach novelty, highly sensitive, fearful, or behaviourally inhibited may be more vulnerable to anxiety.
They may show:
- separation distress,
- school refusal,
- reluctance to speak in groups,
- avoidance of unfamiliar people,
- excessive reassurance seeking,
- somatic complaints before new events.
These children usually benefit from gradual exposure, preparation, predictable routines, parental calmness, and reinforcement of brave behaviour.
Overprotection may unintentionally maintain anxiety. Harsh forcing may worsen fear. The best approach is supported, stepwise mastery.
Temperament and Parenting
Temperament influences parenting experience.
A child with regular routines and mild emotions may make parenting feel easier. A child with irregular sleep, intense emotions, sensory sensitivity, and poor adaptability may make parenting feel exhausting.
This does not mean the parent is failing. It means the parenting strategy must fit the child’s temperament.
| Child Pattern | Less Helpful Response | More Helpful Response |
| High intensity | Shouting, threatening, shaming | Calm limit-setting, co-regulation, emotion naming |
| Slow-to-warm-up | Forcing immediate participation | Preparation, modelling, gradual exposure |
| High distractibility | Repeated verbal scolding | Visual cues, shorter instructions, reduced distractions |
| Low persistence | Calling the child lazy | Breaking tasks into smaller steps, rewarding effort |
| Sensory sensitivity | Dismissing as drama | Identifying triggers, sensory accommodations |
| Irregular routines | Expecting instant discipline | Gradual routine shaping, sleep hygiene, predictable structure |
Temperament-informed parenting is not permissive parenting. The child still needs limits. But limits are delivered in a way that matches the child’s nervous system and developmental capacity.
Clinical Assessment of Temperament
A temperament-informed assessment should include:
| Assessment Area | Key Questions |
| Developmental history | Was the child active, sensitive, irregular, intense, or slow-to-warm from infancy? |
| Sleep and biological rhythm | Are sleep, appetite, and routines predictable or irregular? |
| Response to novelty | Does the child approach or avoid new people, places, foods, and activities? |
| Adaptability | How long does the child take to adjust after change? |
| Sensory profile | Are there sensitivities to sound, light, touch, clothing, food texture, smell, or crowds? |
| Emotional reactivity | How intense are emotional responses? How long does recovery take? |
| Attention and persistence | Can the child sustain effort? Does the child give up quickly? |
| Context | Where does the behaviour occur — home, school, public places, only with certain people? |
| Functional impairment | Is the pattern affecting learning, relationships, family functioning, or daily life? |
| Differential diagnosis | Could ADHD, autism, anxiety, depression, trauma, learning disorder, sleep disorder, or family stress explain the presentation? |
Practical Clinical Formulation
A child’s behavioural difficulty can be formulated through four interacting layers:
| Layer | Example |
| Temperament | High activity, low adaptability, high sensory sensitivity |
| Neurodevelopment | ADHD, autism spectrum traits, learning difficulty |
| Emotional state | Anxiety, depression, irritability, low self-esteem |
| Environment | Parenting style, school demands, family stress, sleep routine, screen exposure |
This layered model is more useful than a single label.
For example, a child who has meltdowns before school may not simply be “stubborn.” The formulation may be:
- low adaptability,
- low sensory threshold,
- anxiety about transitions,
- possible autism spectrum traits,
- poor sleep,
- and a classroom environment that is noisy and unpredictable.
Treatment then becomes targeted and practical.
Management Principles
Temperament-informed intervention includes:
| Goal | Strategy |
| Improve predictability | Use routines, visual schedules, transition warnings |
| Reduce sensory overload | Modify noise, clothing, lighting, crowd exposure |
| Build adaptability | Gradual exposure to change, rehearsal, flexible routines |
| Improve emotional regulation | Emotion labelling, breathing, co-regulation, calming plans |
| Support attention | Short instructions, structured tasks, reduced distractions |
| Improve persistence | Break tasks into steps, reward effort, reduce perfectionistic pressure |
| Improve parent-child fit | Parent training, psychoeducation, consistent but calm boundaries |
| Clarify diagnosis | Assess for ADHD, autism, anxiety, depression, learning disorder, sleep problems |
Temperament Is Not Destiny
Temperament shapes development, but it does not determine destiny.
A highly reactive child can learn emotional regulation.
A slow-to-warm-up child can develop social confidence.
A distractible child can learn structure.
A sensory-sensitive child can learn coping strategies.
A highly persistent child can become disciplined and successful.
An intense child can become passionate, expressive, and creative.
The goal is not to erase temperament. The goal is to help the child use their temperament adaptively.
Conclusion
Thomas and Chess temperament theory remains clinically valuable because it provides a developmental, non-blaming framework for understanding child behaviour.
It reminds us that children differ in activity, rhythm, adaptability, sensory threshold, emotional intensity, mood, attention, and persistence from early life.
These differences interact with parenting, school expectations, culture, stress, and neurodevelopment.
A temperament-informed approach does not ask only, “What diagnosis does this child have?”
It also asks:
“What is this child’s behavioural style?”
“What environment brings out the best or worst in this child?”
“Is there a goodness of fit?”
“What supports can help this child function better?”
This approach allows parents, teachers, and clinicians to move from blame to understanding, and from understanding to effective intervention.
Need Help Understanding Your Child’s Temperament or Behaviour?
If your child is struggling with emotional outbursts, attention difficulties, school refusal, anxiety, sleep problems, sensory sensitivity, social withdrawal, aggression, or repeated behavioural concerns, a structured child and adolescent psychiatric evaluation can help.
Many children are labelled as naughty, stubborn, lazy, oversensitive, or difficult when they may actually be struggling with temperament-related vulnerabilities, ADHD, autism spectrum traits, anxiety, depression, learning difficulties, sleep problems, or family stress.
A proper assessment can help identify the pattern and create a practical plan for the child, parents, and school.
For child behaviour evaluation, ADHD/autism assessment, emotional regulation difficulties, parenting guidance, and treatment planning, consult:
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery, Chennai
Opp. Phoenix Mall
Email: srinivasaiims@gmail.com
Phone: +91-8595155808