Psychosis in Deaf Individuals: Why the Diagnosis Needs Extra Care
 Psychosis is often taught as a condition where a person may hear voices, develop false fixed beliefs, become suspicious, or show disorganised thinking. But when the person is deaf or hard of hearing, the clinical picture becomes more complex. The symptoms may not present in the textbook way, and the risk of misunderstanding is high.
Psychosis is often taught as a condition where a person may hear voices, develop false fixed beliefs, become suspicious, or show disorganised thinking. But when the person is deaf or hard of hearing, the clinical picture becomes more complex. The symptoms may not present in the textbook way, and the risk of misunderstanding is high.
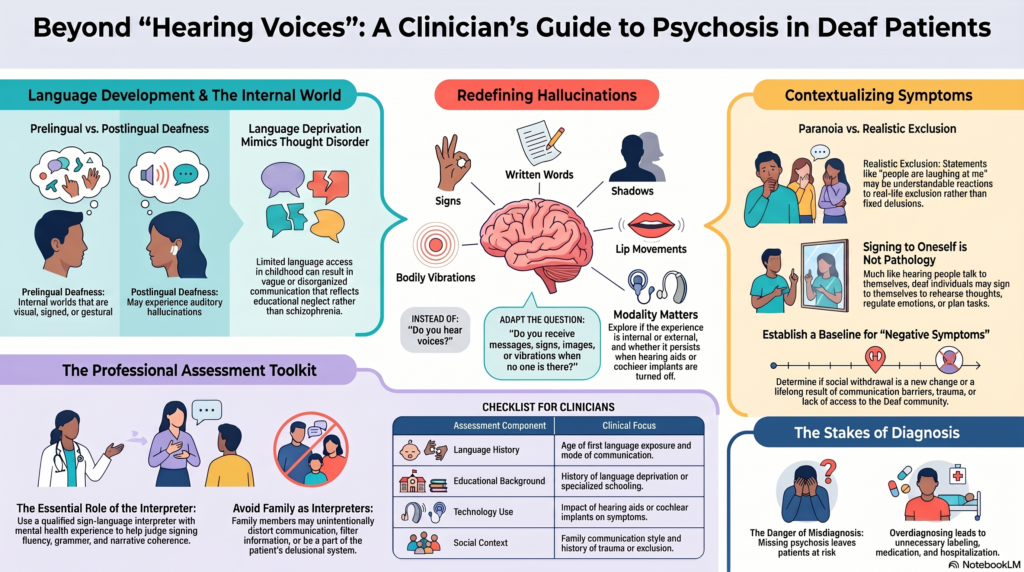
A deaf person with psychosis may not simply say, “I hear voices.” They may describe seeing signs, lip movements, written words, shadows, gestures, vibrations, bodily sensations, or a sense that someone is communicating with them when no one is present. For some, the experience is not a sound but a message. For others, especially those who became deaf later in life or who have residual hearing, the hallucination may still be experienced as a voice or noise.
This is why asking only “Do you hear voices?” is not enough.
A better clinical question is:
“Do you ever receive messages, signs, images, words, vibrations, or sensations when no one is there?”
This small change in questioning can completely change the quality of the assessment.
The First Question: Was Deafness Present Before Language Developed?
One of the most important clinical distinctions is between prelingual and postlingual deafness.
A person who became deaf after learning spoken language may have an inner speech experience similar to hearing individuals. Their hallucinations may still be described in auditory terms.
But a person who was deaf before acquiring language may experience the world very differently. Their internal language may be visual, signed, gestural, spatial, or image-based. If they had delayed access to sign language, they may also have language deprivation. This can create major diagnostic confusion.
Language deprivation can mimic thought disorder.
A patient may appear vague, concrete, poorly organised, or unable to explain experiences clearly. But this may not be schizophrenia. It may reflect limited language access during childhood, educational deprivation, or lack of a shared communication system.
This is one of the most important lessons in assessing psychosis in deaf individuals: poor communication is not automatically disorganised thinking.
Hallucinations May Be Visual, Tactile, Somatic, or Communication-Like
In hearing patients with psychosis, auditory hallucinations are often prominent. In deaf patients, hallucinations may be more visual or bodily.
They may report:
seeing people signing when no one is there,
seeing lips moving without a real person present,
seeing written words or symbols,
feeling vibrations, touch, or bodily sensations,
sensing that someone is sending messages,
or feeling watched, followed, or controlled.
These experiences need to be explored carefully. The clinician should ask about the form, meaning, location, frequency, emotional impact, and level of conviction.
Is it a sound?
Is it an image?
Is it a sign?
Is it a vibration?
Is it a thought?
Is it inside the mind or outside?
Does it happen with hearing aids or cochlear implants on or off?
Without these questions, the clinician may either miss psychosis or diagnose it wrongly.
Paranoia Must Be Understood in Context
Suspiciousness is another area where deaf patients can be misunderstood.
A deaf person may say:
“People are talking about me.”
“They are laughing at me.”
“They are hiding things from me.”
“They don’t tell me what is happening.”
In a hearing person, these statements may immediately raise concern about paranoia. But for a deaf person, these may sometimes be understandable reactions to real-life exclusion.
Many deaf individuals grow up in environments where people speak around them, do not sign, do not include them in conversations, or make decisions without explaining things clearly. Over time, this can create mistrust, anxiety, social withdrawal, or trauma.
So the clinical question is not simply whether the person is suspicious.
The question is whether the belief is fixed, false, disproportionate, bizarre, worsening from baseline, and causing functional impairment.
Good psychiatry requires context. Deaf mental health requires even more context.
Thought Disorder Is Harder to Judge Without Sign Language Expertise
In hearing patients, we assess thought form through speech. In deaf sign-language users, thought form must be assessed through sign language, facial grammar, signing space, sequencing, coherence, and narrative structure.
This is not something a non-signing clinician can reliably judge alone.
A deaf person may use animated facial expressions, body shifts, visual role play, or spatial mapping while signing. To an unfamiliar clinician, this may look odd or exaggerated. But in sign language, it may be completely normal.
Similarly, signing to oneself is not automatically a hallucination. It may be equivalent to talking to oneself, rehearsing thoughts, regulating emotion, remembering tasks, or planning.
The clinician must avoid converting Deaf culture into psychopathology.
The Role of the Interpreter Is Crucial
For proper assessment, a qualified sign-language interpreter is essential. Ideally, the interpreter should have experience in mental health settings.
A family member should not be used as the primary interpreter for a psychiatric evaluation. Family members may filter, simplify, edit, or unintentionally distort the patient’s communication. They may also be part of the conflict or delusional system.
The interpreter can help clarify:
whether the signing is fluent,
whether grammar is unusual,
whether the narrative is coherent,
whether the language appears deprived,
whether there is true disorganisation,
and whether the patient’s communication has changed from baseline.
But the interpreter should not be asked to diagnose. The psychiatrist diagnoses. The interpreter helps preserve the meaning of the patient’s communication.
Negative Symptoms or Social Deprivation?
Another common mistake is overdiagnosing negative symptoms.
A deaf patient may appear withdrawn, quiet, emotionally flat, or socially isolated. But this may be due to lack of accessible communication, depression, bullying, trauma, family exclusion, poor education, or lack of contact with other deaf people.
The key question is change from baseline.
Was the person previously expressive?
Did self-care decline?
Did communication reduce?
Did social interest decrease even when communication was accessible?
Did functioning deteriorate?
Without this timeline, we may mistake lifelong deprivation for illness — or miss a new psychiatric disorder.
A Better Clinical Approach
Assessment of psychosis in deaf individuals should include:
a detailed history of deafness and language development,
mode of communication,
age of first language exposure,
educational background,
family communication style,
hearing aid or cochlear implant use,
neurological history,
substance use history,
trauma history,
collateral information,
and direct observation with a trained interpreter.
The mental status examination should be adapted, not abandoned.
The clinician should explore hallucinations across all modalities, assess delusions in context, understand signing behaviour, and distinguish language deprivation from thought disorder.
Why This Matters
A wrong diagnosis can harm the patient in two ways.
If psychosis is missed, the person may remain untreated, distressed, unsafe, or functionally impaired.
If psychosis is overdiagnosed, the person may be unnecessarily labelled, medicated, hospitalised, or misunderstood for life.
Deaf patients deserve psychiatric care that is not only clinically competent but also linguistically and culturally informed.
The question is not merely, “Does this person have psychosis?”
The better question is:
“Have I understood this person’s language, world, and communication before I interpret their symptoms?”
That is where good psychiatry begins.
For Appointments and Professional Enquiries
Psychiatric symptoms in deaf and hard-of-hearing individuals require careful, respectful, and specialised evaluation. If you or a family member is struggling with suspiciousness, unusual experiences, hallucination-like symptoms, behavioural changes, memory concerns, depression, anxiety, or other psychiatric difficulties, a detailed psychiatric assessment can help clarify what is really happening and guide the right treatment.
Dr. Srinivas Rajkumar T
MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist,
Apollo Clinic Velachery, Chennai, Opp. Phoenix Mall
Email: srinivasaiims@gmail.com
Phone: +91-8595155808