When Alzheimer’s Biomarkers Improve but Patients Do Not : Ceperognastat Trial
 Alzheimer’s disease research is entering an exciting period. New treatments are being developed to target amyloid, tau, inflammation and other biological changes in the brain.
Alzheimer’s disease research is entering an exciting period. New treatments are being developed to target amyloid, tau, inflammation and other biological changes in the brain.
However, a recent clinical trial offers an important reminder:
A medicine can improve blood tests or brain scans without improving the patient’s memory, independence or quality of life.
The medicine studied was ceperognastat, an experimental oral treatment designed to influence tau-related changes in Alzheimer’s disease.
Unfortunately, the treatment did not slow Alzheimer’s disease progression. At the higher dose, some participants experienced greater clinical decline than those receiving placebo.
Why was ceperognastat considered promising?
Alzheimer’s disease is associated with the accumulation of abnormal proteins in the brain.
Two of the best-known proteins are:
- Amyloid, which forms plaques outside brain cells
- Tau, which forms abnormal tangles inside brain cells
The spread of abnormal tau is closely associated with worsening memory, thinking ability and day-to-day functioning.
Ceperognastat blocks an enzyme called O-linked N-acetylglucosaminidase, or OGA. Researchers hoped that blocking this enzyme would change the way tau is processed and reduce the accumulation of harmful tau proteins.
Animal studies had suggested that this approach might reduce tau aggregation and protect brain cells. This led researchers to test the medicine in people with early Alzheimer’s disease.
How was the study conducted?
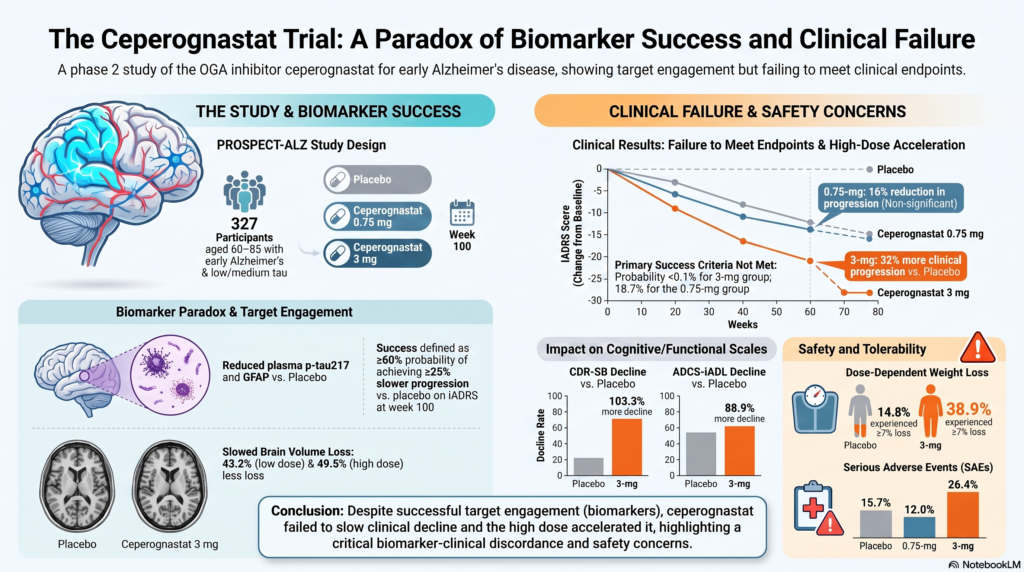
The PROSPECT-ALZ trial included 327 people with early symptomatic Alzheimer’s disease.
Participants received one of three treatments:
- Ceperognastat 0.75 mg daily
- Ceperognastat 3 mg daily
- Placebo
The main analysis focused on people who had low-to-moderate levels of tau on PET brain scans.
Researchers assessed both cognition and daily functioning. They wanted to know whether the medicine could slow the gradual loss of memory, thinking ability and independence.
Did ceperognastat slow Alzheimer’s disease?
No.
After approximately 100 weeks, the lower dose showed a small numerical difference compared with placebo, but the result was not strong enough to demonstrate a meaningful treatment benefit.
The higher dose produced a more concerning result. Participants receiving ceperognastat 3 mg experienced approximately 32% greater clinical progression than those receiving placebo.
The medicine also failed to provide clear benefits on other commonly used Alzheimer’s assessments.
At the higher dose, participants showed significantly greater deterioration in:
- Overall dementia severity
- Instrumental activities of daily living
- Ability to function independently
The decline was particularly noticeable on assessments that included everyday functioning rather than on brief cognitive tests alone.
This distinction is important. A patient may perform reasonably well on a short memory test but still become less able to manage medicines, money, appointments, household tasks or travel.
But some test results appeared encouraging
This is where the study becomes especially interesting.
Although patients did not improve clinically, ceperognastat appeared to influence several Alzheimer’s-related biomarkers.
During treatment, researchers observed:
- Less accumulation of plasma p-tau217
- Lower levels of GFAP, a marker associated with astrocyte activity and inflammation
- A small reduction in tau accumulation in one brain region
- Apparently slower loss of brain volume on MRI
Both doses appeared to reduce whole-brain and hippocampal volume loss compared with placebo during the treatment period.
If we looked only at the scans and blood tests, we might have concluded that the medicine was protecting the brain.
But the patients were not doing better.
At the higher dose, they were doing worse.
How can the brain scan look better while the patient declines?
There are several possible explanations.
1. Changing a biomarker is not the same as treating the disease
A drug may successfully affect its intended biological target without producing a meaningful benefit for the patient.
Ceperognastat probably influenced tau-related biological pathways. The changes in p-tau217, GFAP and tau PET suggest that the medicine was biologically active.
However, influencing one part of Alzheimer’s disease biology may not be enough to preserve memory and independence.
Alzheimer’s disease involves many interacting processes, including:
- Amyloid and tau accumulation
- Inflammation
- Synaptic damage
- Vascular disease
- Metabolic changes
- Mitochondrial dysfunction
- Frailty and physical health
- Sleep, mood and sensory impairment
Improving one laboratory marker may not stop the larger disease process.
2. The target may have been too broad
OGA affects not only tau but also thousands of other proteins throughout the body.
These proteins are involved in basic functions such as metabolism, cell signalling, protein breakdown and cellular survival.
Therefore, strongly blocking OGA may create unwanted effects in the brain or elsewhere in the body. The study authors suggest that possible central or systemic toxicity may have outweighed any anti-tau benefit.
This may help explain why the higher dose was associated with poorer outcomes.
3. Reduced brain shrinkage may not always mean brain protection
MRI brain volume is useful, but it does not measure the number of healthy functioning neurons directly.
Brain volume can also be influenced by:
- Fluid shifts
- Inflammation
- Changes in cellular size
- Changes in blood vessels
- Changes in tissue water content
The researchers therefore suggested that the apparent preservation of brain volume might have reflected fluid or cellular-volume changes rather than true neuroprotection.
After the medicine was stopped, the MRI differences between the groups disappeared.
What about side effects?
Serious adverse events were more frequent in the higher-dose group.
A serious adverse event occurred in:
- 12% of participants receiving 0.75 mg
- 26.4% receiving 3 mg
- 15.7% receiving placebo
Weight loss was another important finding.
At least 7% body-weight loss occurred in:
- 34% of the lower-dose group
- 38.9% of the higher-dose group
- 14.8% of the placebo group
Weight loss can be particularly harmful in older adults. It may contribute to weakness, falls, muscle loss, frailty and reduced ability to perform daily activities.
Weight improved after the medicine was discontinued, suggesting that this effect was at least partly reversible.
What happened after treatment was stopped?
A smaller group of participants was followed for approximately nine months after treatment ended.
There was no delayed clinical benefit.
The earlier differences in brain volume and blood biomarkers gradually disappeared. The group that had received the higher dose continued to show poorer scores on at least one measure of dementia severity.
Because fewer people participated in this follow-up, the results must be interpreted cautiously. However, the follow-up did not reveal a hidden or delayed benefit.
Does this mean that tau is not an important target?
No.
Tau remains one of the most important biological targets in Alzheimer’s disease research.
The study does not show that all tau treatments will fail. It shows that OGA inhibition with ceperognastat was not an effective way to slow early symptomatic Alzheimer’s disease.
Other tau treatments may work differently, such as by:
- Preventing abnormal tau aggregation
- Reducing production of harmful tau
- Blocking the spread of tau between brain cells
- Improving clearance of abnormal tau
- Targeting more specific toxic forms of tau
A failed treatment can still help researchers understand which approaches are less likely to succeed.
What should patients and families learn from this study?
Whenever a new Alzheimer’s treatment is reported, it is useful to ask:
- Did patients actually decline more slowly?
- Did they remain independent for longer?
- Was the benefit noticeable in daily life?
- What side effects occurred?
- Did the benefits continue over time?
Statements such as “reduced tau,” “improved brain volume” or “changed a blood biomarker” are scientifically interesting.
But they do not automatically mean that the treatment improves the patient’s life.
The most important lesson
The ceperognastat trial highlights the difference between biological activity and clinical benefit.
The medicine altered some Alzheimer’s biomarkers and appeared to reduce brain-volume loss during treatment. Yet it did not protect cognition or daily functioning. At the higher dose, patients experienced greater clinical decline.
The goal of Alzheimer’s treatment is not simply to produce a better scan.
It is to help the person:
- Remember better
- Function independently
- Remain socially connected
- Experience a better quality of life
- Reduce dependence on caregivers
- Preserve dignity for as long as possible
Biomarkers are valuable tools, but the patient must remain at the centre of dementia research.
Reference
Fleisher AS, Munsie L, Mancini M, et al. Ceperognastat in Early Symptomatic Alzheimer Disease: A Randomized Clinical Trial. JAMA. Published online July 13, 2026. doi:10.1001/jama.2026.12768.
About the Author
Dr. Srinivas Rajkumar T
MD Psychiatry(AIIMS New Delhi)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery, Chennai
Opposite Phoenix Marketcity
Email: srinivasaiims@gmail.com
Phone: +91-8595155808
Dr. Srinivas provides assessment and treatment for memory complaints, mild cognitive impairment, dementia, behavioural symptoms associated with dementia and other neuropsychiatric conditions.
This article is for public education and does not replace an individual medical consultation.