ADHD, Dyslexia and Dementia Risk in Older Women: What Happens to Childhood Neurodevelopmental Differences With Age?
 An older woman recently spoke to me about the difficulties she had experienced since childhood. Reading had always required extra effort. She struggled to remain attentive, organise tasks and remember instructions. Yet she had completed her education, managed her family responsibilities and built a meaningful life—largely by working harder and developing her own coping strategies.
An older woman recently spoke to me about the difficulties she had experienced since childhood. Reading had always required extra effort. She struggled to remain attentive, organise tasks and remember instructions. Yet she had completed her education, managed her family responsibilities and built a meaningful life—largely by working harder and developing her own coping strategies.
Now, in later life, she had a different question:
“What will happen to me in the future? Am I more likely to develop dementia?”
This is an increasingly important question. Many women who grew up several decades ago were never assessed for attention-deficit/hyperactivity disorder, dyslexia or other neurodevelopmental conditions. Their difficulties were often attributed to laziness, carelessness, nervousness, poor motivation or lack of intelligence.
Only after retirement—or after their children or grandchildren receive a diagnosis—do they begin to recognise that their lifelong struggles may have had a name.
Neurodevelopmental conditions do not disappear at adulthood
ADHD, dyslexia, autism, developmental coordination disorder and other specific learning disorders begin during childhood. They may change in appearance with age, but they do not automatically disappear when someone finishes school.
A child who constantly moved around the classroom may become an adult who experiences internal restlessness. A girl who quietly daydreamed may become a woman who repeatedly forgets appointments, loses objects, procrastinates or becomes overwhelmed by domestic and professional responsibilities.
Similarly, childhood dyslexia may later appear as:
- Slow or effortful reading
- Difficulty following lengthy written instructions
- Spelling problems
- Avoidance of paperwork
- Difficulty learning unfamiliar names or technical terms
- Reliance on memory, context or other people to compensate
These individuals may nevertheless become highly successful. Intelligence, creativity, social skills and practical reasoning can allow them to compensate for weaknesses in attention, reading or working memory.
How common is undiagnosed ADHD in older adults?
Global analyses suggest that approximately 2.6% of adults have persistent ADHD originating in childhood, while a larger proportion experience clinically significant ADHD symptoms without clearly documented childhood histories.
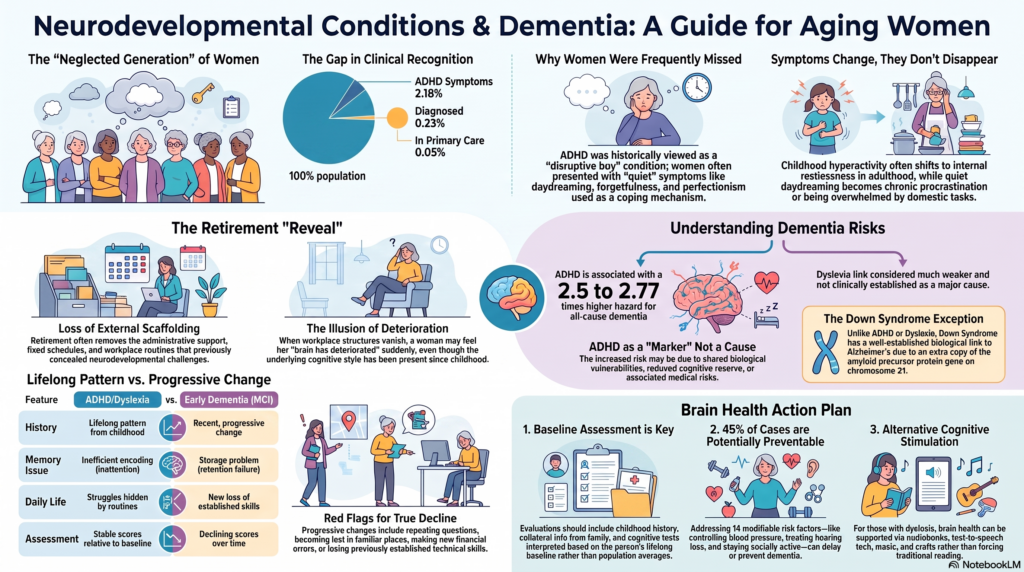
In older adults, the difference between research estimates and actual clinical recognition is striking. A systematic review found ADHD-like symptoms in approximately 2.18% of older adults, but only 0.23% had a recorded clinical diagnosis, and just 0.09% were receiving ADHD treatment.
A large English primary-care analysis published in 2026 found that only 0.05% of people over 65 had ADHD recorded in their medical records—far below expected population prevalence. This does not prove that every older person reporting inattention has ADHD, but it strongly suggests that ADHD has historically been overlooked in later life.
Why were so many women missed?
For many years, ADHD was imagined primarily as a condition affecting hyperactive and disruptive schoolboys.
Girls and women are more likely to present with less visible difficulties such as:
- Daydreaming and mental wandering
- Disorganisation
- Forgetfulness
- Emotional sensitivity
- Chronic procrastination
- Feeling mentally overwhelmed
- Anxiety caused by repeated mistakes
- Excessive perfectionism developed as compensation
Because these women were not disturbing the classroom, they were less likely to be referred for assessment. Their difficulties were frequently interpreted as anxiety, depression, low confidence or inadequate effort.
Research consistently shows that females are less likely to be diagnosed during childhood and commonly receive their diagnosis later than males.
Older women represent a particularly neglected generation. Many attended school before ADHD and specific learning disorders were widely understood. Educational systems frequently punished poor performance without investigating its neurodevelopmental basis.
Dyslexia may also remain hidden for a lifetime
Developmental dyslexia affects reading accuracy, fluency, spelling and the rapid processing of written language. A worldwide meta-analysis estimated its prevalence among schoolchildren at approximately 7%, although estimates vary depending on the language, definition and testing method used.
There is no reliable global estimate of how many older adults with dyslexia remain undiagnosed. Nevertheless, it is reasonable to assume that the proportion is substantial because structured assessments and educational accommodations were rarely available when today’s elderly population attended school.
Some people compensated by choosing practical occupations, memorising information, asking relatives to handle written documents or avoiding situations that exposed their reading difficulties.
Why do lifelong difficulties sometimes feel worse after retirement?
Retirement does not usually cause ADHD or dyslexia. Instead, it can remove the external structure that previously concealed them.
During working life, the person may have had:
- A fixed daily schedule
- Secretarial or administrative support
- Repeated familiar tasks
- Regular social contact
- A spouse managing finances or appointments
- Strong routines developed over several decades
After retirement, bereavement, relocation or changes in family structure, those supports may disappear. Sleep problems, depression, loneliness, medical illness, hearing loss, medication effects and reduced physical activity can further worsen attention and memory.
The result may be a sudden feeling that “my brain has deteriorated,” even when part of the difficulty has been present since childhood.
Does ADHD increase the risk of dementia?
Recent evidence suggests that adults diagnosed with ADHD may have a higher rate of later dementia. However, this must be explained carefully.
A 2026 systematic review and meta-analysis found that people with ADHD had approximately 2.5 times the hazard of developing all-cause dementia compared with people without ADHD. The authors nevertheless emphasised that the available studies were limited and that the results did not establish that ADHD directly causes dementia.
In a major Israeli cohort study involving 109,218 adults followed for more than 17 years, dementia was diagnosed in 13.2% of participants with adult ADHD, compared with 7% of those without ADHD. After adjustment for multiple health and demographic factors, adult ADHD was associated with a 2.77-fold higher dementia hazard.
These figures represent a group-level association, not an individual prediction. They do not mean that a person with ADHD has a 2.5-fold certainty of developing dementia.
Several explanations remain possible:
Shared biological vulnerability
ADHD and some dementias may share genetic, neurochemical or brain-network vulnerabilities. These pathways remain under investigation.
Reduced cognitive reserve
A lifetime of educational difficulty, inconsistent cognitive stimulation or occupational disadvantage could reduce the brain’s capacity to compensate for age-related pathology.
Associated medical risks
People with untreated ADHD may have higher rates of smoking, obesity, hypertension, diabetes, sleep disturbance, depression, substance misuse and physical inactivity. Several of these are independently recognised dementia risk factors.
Diagnostic overlap
Early cognitive decline can resemble ADHD, particularly when an older adult receives an ADHD diagnosis for the first time. Some apparent “late ADHD” may represent the early stages of another cognitive disorder.
Greater healthcare contact
People diagnosed with ADHD may be monitored more closely, making dementia more likely to be recognised and recorded.
Therefore, ADHD should currently be considered a possible marker of increased vulnerability, rather than a proven direct cause of dementia.
Does ADHD treatment prevent dementia?
The Israeli cohort found no clear increase in dementia risk among participants with ADHD who had received psychostimulant medication. This is scientifically interesting, but it does not prove that stimulants prevent dementia. The treated subgroup was relatively small, and people receiving treatment may differ from untreated patients in several other ways.
Stimulants should therefore not be prescribed as dementia-prevention medicines. In older adults, treatment decisions must consider blood pressure, cardiac health, sleep, anxiety, appetite, other medications and the degree of functional impairment.
Nevertheless, appropriately treating ADHD may improve organisation, medication adherence, driving safety, emotional regulation and the ability to maintain healthy routines—all of which can indirectly support long-term brain health.
Does dyslexia cause Alzheimer’s disease?
The evidence is much weaker than it is for ADHD.
A 2024 genetic study using Mendelian randomisation reported a small association between genetic liability to dyslexia and Alzheimer’s disease, with an estimated odds ratio of approximately 1.15. However, the association was no longer statistically significant after accounting for cognitive performance, and no clear relationship was found with vascular, Lewy body or frontotemporal dementia.
This is an early genetic finding, not sufficient evidence to tell a patient that dyslexia causes dementia.
The more clinically relevant issue is that lifelong dyslexia can complicate dementia assessment. Someone who has always read slowly, struggled with spelling or performed poorly on language-heavy tests may obtain a low cognitive-screening score even when there has been no neurodegenerative decline.
Clinicians must compare current functioning with the person’s own lifelong baseline rather than simply comparing the person with population averages.
What about other neurodevelopmental conditions?
Research into ageing among autistic adults is still developing. A 2026 study of adults aged 65 and above found a modestly higher adjusted risk of diagnosed neurocognitive disorders among autistic adults. However, diagnostic practices, associated medical conditions and intellectual disability can influence these findings.
Down syndrome is an important exception where the connection with Alzheimer’s disease is well established. The extra copy of chromosome 21 includes the amyloid precursor protein gene, creating a strong biological vulnerability. Nearly all people with Down syndrome develop Alzheimer-type brain pathology by around 40, although clinical dementia develops later and not at the same age in every person.
For autism without intellectual disability, dyslexia, developmental coordination disorder and most other neurodevelopmental differences, current evidence is not strong enough to provide precise individual dementia-risk estimates.
ADHD, dyslexia or early dementia: how do we tell the difference?
The most important question is not simply, “Does this person forget things?”
It is:
“Is this a lifelong pattern, or is it a progressive change from the person’s previous level of functioning?”
ADHD and dyslexia generally produce longstanding patterns. The person may remember similar difficulties at school, college, work and home.
Possible dementia becomes more concerning when there is a progressive change such as:
- Repeating the same questions
- Forgetting recently learned information despite paying attention
- Becoming lost in familiar places
- Making new financial errors
- Losing previously established cooking or technical skills
- Difficulty recognising familiar people or objects
- Increasing dependence in everyday activities
- Clear deterioration noticed by family members
Research comparing older adults with ADHD and mild cognitive impairment found that memory problems in ADHD were more consistent with inefficient encoding—information was not registered properly because of attention difficulties. In mild cognitive impairment, the pattern was more consistent with a storage problem, meaning information was learned but not retained normally.
This distinction cannot be established from one symptom or one screening score. It requires a detailed developmental history, collateral information, functional assessment and appropriately interpreted cognitive testing.
What should an older adult with lifelong ADHD or dyslexia do?
The answer should not be panic. It should be baseline assessment, prevention and monitoring.
A useful evaluation may include:
- A detailed childhood, educational and occupational history
- Information from a spouse, sibling or adult child
- Assessment of current daily functioning
- Cognitive testing interpreted according to language and educational background
- Screening for depression, anxiety and sleep disorders
- Review of medications that may impair cognition
- Evaluation of hearing, vision, thyroid function, vitamin deficiencies and vascular health
People with dyslexia may require tests that minimise unnecessary dependence on reading and written language. A single low MoCA or MMSE score should never be interpreted without considering education, literacy, language and lifelong learning difficulties.
Protecting the future brain
Having ADHD or dyslexia does not make dementia inevitable. A person’s future risk is influenced by many interacting biological, medical and social factors.
The 2024 Lancet Commission estimated that approximately 45% of dementia cases could potentially be prevented or delayed by addressing 14 modifiable risk factors across the lifespan.
For an older adult with ADHD or another neurodevelopmental condition, a practical brain-health plan should particularly focus on:
- Controlling blood pressure, diabetes and LDL cholesterol
- Regular aerobic and strength exercise
- Treating depression and persistent anxiety
- Identifying sleep apnoea and chronic sleep deprivation
- Correcting hearing and vision loss
- Avoiding smoking and excessive alcohol
- Preventing head injury
- Maintaining friendships and meaningful social roles
- Continuing cognitively stimulating activities
- Using calendars, alarms, written routines and pill organisers
- Reviewing medications regularly
- Seeking assessment when there is a genuine change from baseline
Reading can remain cognitively valuable, but a person with dyslexia need not force herself to use only traditional printed material. Audiobooks, text-to-speech technology, discussion groups, music, language learning, puzzles, teaching, crafts and other intellectually engaging activities can also provide sustained cognitive stimulation.
What can we honestly tell the patient?
We can say:
“Your childhood ADHD or dyslexia did not suddenly become dementia. These are lifelong neurodevelopmental differences. ADHD may be associated with a higher average risk of later cognitive impairment, but it does not determine your future. Dyslexia itself has not been established as a major clinical cause of dementia. What matters now is documenting your baseline, identifying any true progression and aggressively protecting your physical, emotional and cognitive health.”
For many older women, receiving a neurodevelopmental explanation is not merely about acquiring a diagnostic label. It can replace decades of shame with understanding.
The goal is not to reinterpret every past difficulty as illness. The goal is to recognise the person’s lifelong cognitive style, distinguish it from new decline and create a realistic plan for healthy ageing.
Dr. Srinivas Rajkumar T
MD Psychiatry(AIIMS New Delhi)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery, Chennai
Opposite Phoenix Marketcity
Email: srinivasaiims@gmail.com
Phone: +91-8595155808
Assessment services include adult ADHD evaluation, computerised cognitive assessment and evaluation of memory concerns in older adults. This article is intended for public education and does not replace an individual clinical assessment.