ADHD is Not One Disorder: Understanding the 3 Brain-Based Biotypes
 Attention-Deficit/Hyperactivity Disorder (ADHD) is often spoken about as if it is a single condition. In reality, anyone who has worked clinically with ADHD knows this is far from true.
Attention-Deficit/Hyperactivity Disorder (ADHD) is often spoken about as if it is a single condition. In reality, anyone who has worked clinically with ADHD knows this is far from true.
Some individuals struggle with restlessness and impulsivity. Others seem quiet, inattentive, and mentally “elsewhere.” A third group presents with emotional volatility—irritability, mood swings, and difficulty regulating feelings.
The question is:
Are these just different presentations of the same disorder, or are they fundamentally different conditions?
A recent study published in JAMA Psychiatry (2026) takes us closer to an answer. Using advanced brain imaging and data-driven clustering, researchers identified three distinct ADHD biotypes, each with its own neural signature and clinical profile.
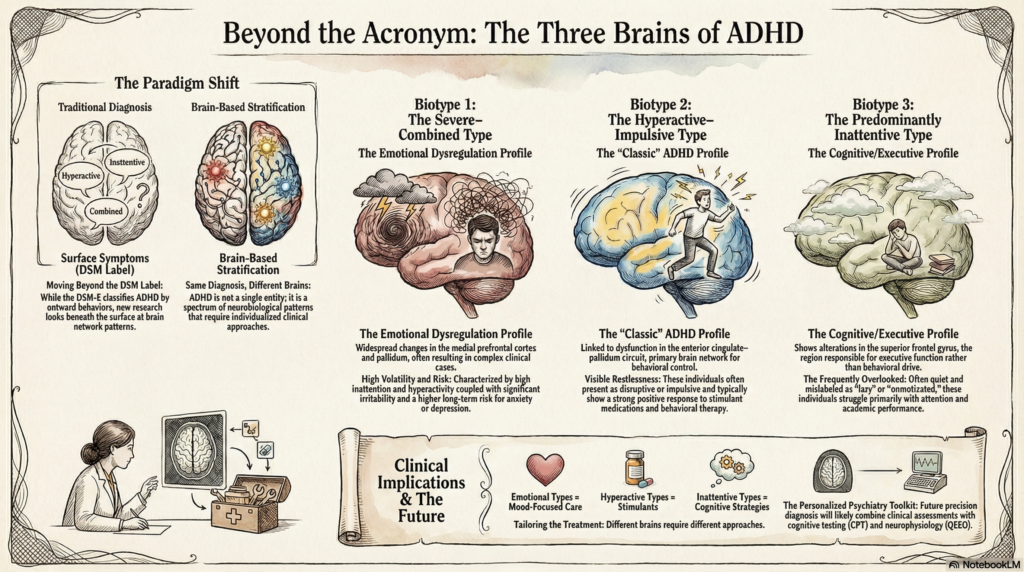
Moving Beyond DSM Labels
The DSM-5 classifies ADHD into:
- Inattentive type
- Hyperactive-impulsive type
- Combined type
While useful, this classification is based purely on observable symptoms.
However, symptoms are the surface.
What this study shows is that beneath these symptoms lie different brain network patterns.
In other words:
ADHD is not one disorder—it is a group of related conditions with different underlying neurobiology.
The 3 ADHD Biotypes (A Brain-Based View)
1. The Severe–Combined Type with Emotional Dysregulation
This group shows widespread brain network changes, particularly involving the medial prefrontal cortex and pallidum.
Clinical Features:
- High inattention
- High hyperactivity and impulsivity
- Significant emotional dysregulation (irritability, mood swings)
Clinical Insight:
These individuals often present as “complex cases.”
They may be misdiagnosed with mood disorders or personality-related issues.
Importantly, this group tends to have:
- More persistent symptoms
- Higher risk of developing anxiety or depression over time
2. The Hyperactive–Impulsive Type
This biotype is linked to dysfunction in the anterior cingulate–pallidum circuit, a key network for behavioral control.
Clinical Features:
- Prominent hyperactivity
- Impulsivity
- Relatively less inattention
Clinical Insight:
This is the “classic ADHD” many people recognize:
- Restless
- Disruptive
- Acting without thinking
These individuals often respond well to stimulant medications and behavioral interventions.
3. The Predominantly Inattentive Type
This group shows alterations in the superior frontal gyrus, a region associated with executive function.
Clinical Features:
- Poor attention
- Low hyperactivity
- Often quiet and overlooked
Clinical Insight:
These individuals are frequently missed in early diagnosis:
- They may be labeled as “lazy” or “unmotivated”
- Academic difficulties are common
This is fundamentally a cognitive/executive dysfunction profile, rather than a behavioral one.
Why This Matters in Clinical Practice
1. Explains Variable Treatment Response
Not all ADHD patients respond the same way to treatment—and this is why.
- Emotional dysregulation type → may need mood-focused interventions
- Hyperactive type → responds well to stimulants
- Inattentive type → may benefit more from cognitive strategies
2. Moves Toward Personalized Psychiatry
This study represents a shift from:
- Symptom-based diagnosis → Brain-based stratification
In the future, combining:
- Clinical assessment
- Cognitive testing (CPT)
- Neurophysiology (QEEG)
may allow us to identify individual ADHD profiles more precisely.
3. Reframes ADHD for Patients and Families
Understanding ADHD as a heterogeneous condition helps reduce stigma.
Instead of asking:
“Why can’t this person just focus?”
We begin to ask:
“What kind of ADHD does this person have, and what support do they need?”
The Bigger Takeaway
The most important message from this research is simple:
Same diagnosis does not mean same brain.
ADHD is not a single entity—it is a spectrum of neurobiological patterns, each requiring a slightly different approach.
Recognising this is the first step toward:
- Better diagnosis
- More targeted treatment
- Improved long-term outcomes
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808