How to Handle “Difficult” Children – Systems-level guide for parents
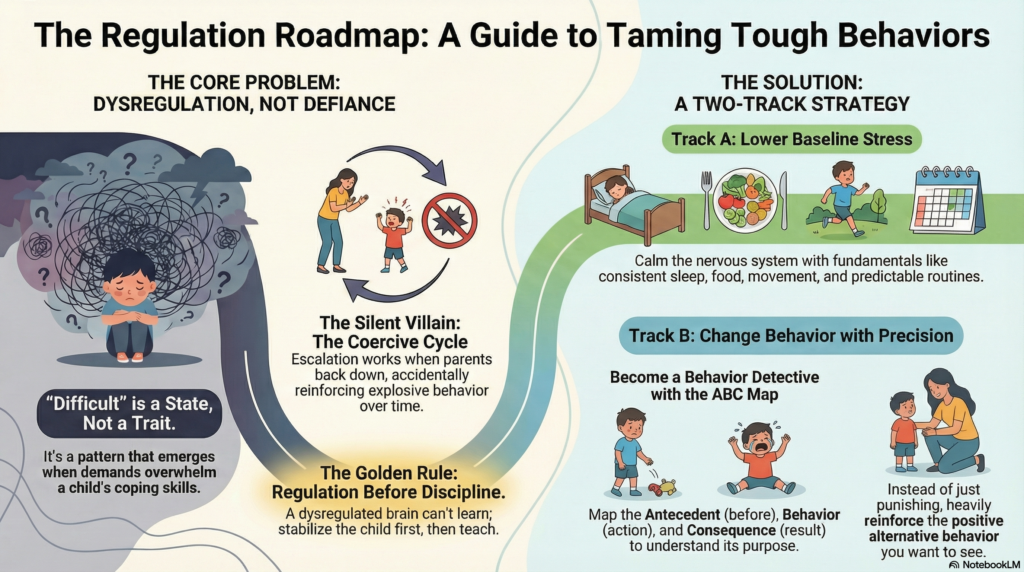 “Difficult” is rarely a personality type. It’s usually a pattern: big reactions, low frustration tolerance, explosive refusals, or relentless negotiation—often worse in the evenings, around transitions, or when screens are involved.
“Difficult” is rarely a personality type. It’s usually a pattern: big reactions, low frustration tolerance, explosive refusals, or relentless negotiation—often worse in the evenings, around transitions, or when screens are involved.
A more accurate framing is this:
A child becomes “difficult” when demands exceed skills, and the nervous system keeps getting pushed into “fight / flight / freeze.” That state can become the child’s new normal through allostasis (the brain’s way of adapting to stress), and over time can build allostatic load—the wear-and-tear of living on high alert. (1)
This article blends: Indian clinical parenting wisdom from Dr. Shekhar Seshadri (calm boundaries, dignity, realism), behavior science (how patterns get reinforced), developmental neuroscience (regulation before reasoning), and evidence-based parenting programs that consistently work.
1) Start with the right model: regulation, not morality
When a child is dysregulated, the “thinking brain” is less available. In that state, long lectures don’t teach; they irritate. The practical implication is simple:
Regulation comes before discipline.
That doesn’t mean “no boundaries.” It means: stabilize first, teach second, consequences last.
2) The silent villain: coercive cycles (how homes accidentally train explosions)
Many families get stuck in what coercion theory describes:
Parent makes a demand → child escalates → parent backs off to stop the chaos → child learns that escalation works → parent learns that giving in ends pain. The pattern strengthens with repetition. (2)
This is why a child may appear to “improve” when parents stop asking—because the system has learned avoidance, not skills.
Your job is to break the learning loop without breaking the relationship.
3) What actually has strong evidence: Parent Management Training and its cousins
Across disruptive behaviors (aggression, severe noncompliance, oppositional patterns), the most consistent evidence supports behavioral parent training / parent management training (PMT): changing triggers, reinforcement, routines, consistency, and parent-child interaction patterns. (3)
Major, well-studied approaches include:
-
PMT (Kazdin and others) for oppositional/aggressive behavior (3)
-
Triple P (multi-level parenting support system) (4)
-
Incredible Years (strong meta-analytic evidence) (5)
-
Parent–Child Interaction Therapy (PCIT) (meta-analytic evidence; consistent benefits across settings) (6,7)
The shared DNA across these programs is not “being strict.” It’s predictability + reinforcement + relationship repair.
4) A useful two-track strategy (that prevents burnout)
Think like a clinician designing a plan:
Track A: Lower baseline stress (allostatic load reduction)
If the child’s nervous system is constantly running hot, every request feels like an attack. Reduce baseline arousal with boring-but-powerful fundamentals:
-
Sleep anchoring (consistent bedtime/wake time, wind-down routine)
-
Food timing (many “behavior problems” are hunger + fatigue in disguise)
-
Predictable transitions (warnings, visual schedules, fewer surprises)
-
Movement (daily vigorous activity is an underrated regulator)
These are not “soft.” They are neurobiology-friendly.
Track B: Change behavior with behavioral precision (without drama)
Use behavioral science without turning your house into a police state:
-
Define one target behavior (observable, specific)
-
Reinforce the alternative behavior heavily at first
-
Keep consequences brief, consistent, and unemotional
5) The ABC map: become a behavior detective, not a judge
Before you “fix” behavior, understand it:
-
A: Antecedent (what happens right before?)
-
B: Behavior (what exactly did the child do?)
-
C: Consequence (what did the child gain or avoid?)
Most challenging behaviors function to:
-
escape a demand
-
gain attention (even negative attention counts)
-
access a preferred activity
-
regulate internal distress
Once you see the function, you stop fighting shadows.
6) The workhorse technique: differential reinforcement (teach the replacement)
PMT relies heavily on reinforcing what you want instead of only punishing what you don’t want. (3)
Examples:
-
If the child screams when denied: reinforce “asking in a calm voice”
-
If homework triggers refusal: reinforce starting for 3 minutes (not just finishing)
This is skill-building disguised as discipline.
7) “Reverse shaping” (a practical term) — build success backwards
You asked for this concept: here’s the sophisticated version.
Reverse shaping = start by making success easy, then gradually raise expectations.
In behavior analysis terms, you’re manipulating task difficulty, reinforcement density, and thresholds so the child experiences repeated wins.
Example: bedtime chaos
-
First target: child enters bedroom without argument
-
Next: pajamas + teeth
-
Next: lights off with parent present
-
Next: parent exits for 2 minutes… then 5… then 10
You are fading supports as regulation improves.
8) “Alternate high” — replace the reward, don’t wrestle it
Some children (especially those with attention/impulsivity traits) become dependent on fast rewards: screens, fights, sarcasm, control battles. If you remove the reward without replacing it, the system panics.
Alternate high = creating a healthier, equally compelling reward channel:
-
intense movement (sports, swimming, cycling)
-
mastery-based flow (music, art, robotics, building)
-
real social reward (teams/clubs with structure)
-
meaningful responsibility (short, winnable jobs that earn status)
This is especially important when screens have become the child’s main emotion regulator.
9) Screens as “emotion medication”: where behavioral addiction principles help
The WHO defines gaming disorder in ICD-11 as impaired control, priority over other activities, and continuation/escalation despite negative consequences. (8) Not every heavy gamer has a disorder—but the definition is useful because it highlights loss of control and functional impairment, not moral panic.
A pragmatic, pediatric-friendly approach supported by the American Academy of Pediatrics is to create a Family Media Plan: clear rules for timing, zones (bedroom/dining), and priorities (sleep, school, relationships). (9,10)
If screens are fueling dysregulation:
-
reduce frictionless use (autoplay, endless short videos, notifications)
-
create stopping points (one episode, one match)
-
move devices out of bedrooms (protect sleep)
-
increase alternate highs (see above)
-
expect a short-term spike in irritability if the child was using screens to self-soothe
10) Emotion coaching: validate feelings without surrendering the boundary
Gottman’s work on parental meta-emotion and “emotion coaching” emphasizes helping children name and navigate emotions rather than dismissing or escalating them. (11)
The key script is:
“I get the feeling. The limit stays.”
Examples:
-
“You’re furious. I understand. And we’re still leaving now.”
-
“You really want more screen time. It’s hard to stop. Time is up.”
This reduces shame, preserves connection, and still holds structure.
11) The Indian clinical realism (Seshadri’s spine + softness)
In Indian families, the environment includes grandparents, school pressure, comparison culture, and limited time. Dr. Shekhar Seshadri’s parenting message (in his public parenting discussions and writings) consistently points toward calm authority: boundaries with dignity, reduced power struggles, and an emphasis on what the child is communicating through behavior. (12,13)
The spirit is:
-
Don’t humiliate.
-
Don’t negotiate endlessly.
-
Don’t escalate.
-
Be consistent enough that the child stops testing reality every day.
A child who trusts the boundary spends less energy fighting it.
12) When it’s not “parenting,” it’s a treatable condition
If difficult behavior is persistent and impairing, screen for:
-
ADHD, anxiety, learning disorder
-
autism traits / sensory sensitivity
-
sleep disorders
-
mood dysregulation
-
family stressors (conflict, inconsistency, trauma)
Evidence-based parenting works even more effectively when underlying issues are identified early.
A compact “starting plan” (the next 2 weeks)
-
Pick one target behavior
-
Do ABC mapping for 7 days
-
Start daily 10 minutes child-led connection (no teaching, no correcting)
-
Reinforce one alternative behavior (small, frequent rewards)
-
Tighten one routine (sleep or homework) with reverse shaping
-
Reduce one screen risk (bedroom devices or autoplay) using the Family Media Plan idea
This is how chaos becomes data, and data becomes change.
References :
-
McEwen BS. Stress, adaptation, and disease: allostasis and allostatic load. Ann N Y Acad Sci. 1998;840:33-44.
-
Patterson GR. Coercive Family Process. Eugene (OR): Castalia Publishing Company; 1982.
-
Kazdin AE. Parent management training: evidence, outcomes, and issues. J Am Acad Child Adolesc Psychiatry. 1997;36(10):1349-56.
-
Sanders MR. The Triple P system of evidence-based parenting support: past, present, and future directions. Child Adolesc Psychiatry Ment Health. 2023;17:1-19.
-
Menting ATA, de Castro BO, Matthys W. Effectiveness of the Incredible Years parent training to modify disruptive and prosocial child behavior: a meta-analytic review. Clin Psychol Rev. 2013;33(8):901-13.
-
Thomas R, Zimmer-Gembeck MJ. Parent-child interaction therapy: a meta-analysis. Pediatrics. 2017;140(3):e20170352.
-
Valero-Aguayo L, Rodríguez-Bocanegra M, Ferro-García R, Ascanio-Velasco L. Meta-analysis of the efficacy and effectiveness of parent-child interaction therapy (PCIT). Psicothema. 2021;33(4):544-52.
-
World Health Organization. Gaming disorder. ICD-11: disorders due to addictive behaviours. Geneva: WHO; 2020.
-
American Academy of Pediatrics. AAP Family Media Plan. HealthyChildren.org. Updated 2024.
-
American Academy of Pediatrics. How to make a family media use plan. HealthyChildren.org. Updated 2024.
-
Gottman JM, Katz LF, Hooven C. Parental meta-emotion philosophy and the emotional life of families: theoretical models and preliminary data. J Fam Psychol. 1996;10(3):243-68.
-
Seshadri S, Rao N. Parenting: The Art and Science of Nurturing. New Delhi: Byword Books; 2012.
-
ParentCircle. Parenting Pathshala series featuring Dr Shekhar Seshadri (NIMHANS): setting healthy boundaries and related parenting guidance. ParentCircle; 2020.
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist,
Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
Related posts:
- How Parents Can Handle Screen Addiction in Children
- Supporting Parents and Caregivers of Children with Autism
- 🌟 Psychiatric Medicines in Children – Myths, Misconceptions & The Truth Parents Need to Know
- ⏳ Developmental Delay in Children – Early Signs, Causes, Screening & What Parents Should Do
- 🧩 Managing Sensory Issues in Autism: A Practical Guide for Parents
- School Refusal: Causes, Signs, and How Parents Can Help