Melatonin Timing: A Scientific and Clinical Perspective Beyond “Take It at Bedtime”
 Melatonin is among the most misunderstood molecules in clinical medicine.
Melatonin is among the most misunderstood molecules in clinical medicine.
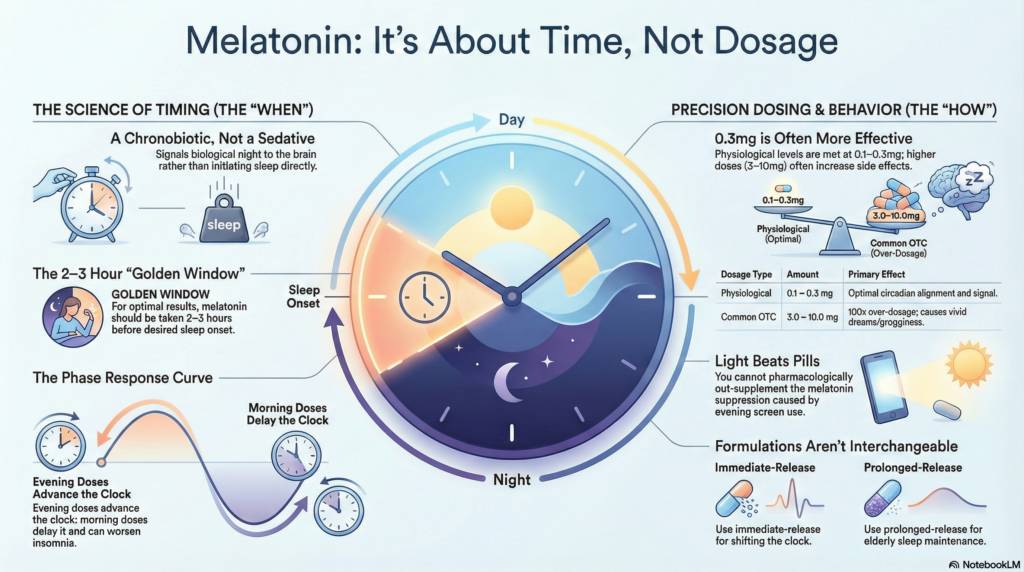
It is sold as a sleeping pill, prescribed as a sedative, and consumed casually—yet its true role is neither hypnotic nor anxiolytic. Melatonin is fundamentally a circadian signal, and its clinical effects depend far more on when it is taken than how much is taken.
Understanding melatonin properly requires stepping back into chronobiology.
Melatonin Is a Time Cue, Not a Sleep Drug
Endogenous melatonin is secreted by the pineal gland under the control of the suprachiasmatic nucleus (SCN)—the brain’s master circadian clock. Its release begins in dim light conditions and peaks during the biological night.
Crucially:
-
Melatonin does not initiate sleep directly
-
It signals biological night to peripheral and central clocks
-
Sleep occurs when melatonin secretion aligns with homeostatic sleep pressure
This is why melatonin is best described as a chronobiotic—an agent that shifts or stabilizes circadian phase.
Dim Light Melatonin Onset (DLMO): The Missing Concept in Clinical Practice
The most important physiological marker in melatonin biology is Dim Light Melatonin Onset (DLMO)—the time at which endogenous melatonin first begins to rise in the evening.
In most adults:
-
DLMO occurs 2–3 hours before habitual sleep onset
-
Sleep typically begins after melatonin has already been rising for some time
Exogenous melatonin works best when administered before or around DLMO, not after it.
This is the scientific reason bedtime dosing often fails.
The Phase Response Curve (PRC): Why Timing Can Help or Harm
Melatonin follows a Phase Response Curve, meaning:
-
Early evening dosing → advances the circadian clock (earlier sleep)
-
Morning dosing → delays the clock (later sleep)
-
Late-night dosing → minimal benefit, more side effects
Clinically relevant implication:
The same dose of melatonin can either correct delayed sleep—or worsen it—depending on timing.
This is rarely explained to patients and inconsistently applied in practice.
Optimal Timing: A Biological, Not Clock-Time Decision
For most adults:
-
Best window: 2–3 hours before desired sleep onset
-
For delayed sleep phase: 3–5 hours before habitual sleep time
-
Consistency matters more than precision
Melatonin taken at bedtime often misses the phase-shifting window and functions only as a weak sedative—if at all.
Dose–Response: Why Higher Is Not Better
Physiological nocturnal melatonin levels are achieved with doses as low as 0.1–0.3 mg.
Common over-the-counter doses (3–10 mg):
-
Exceed physiological levels by 10–100×
-
Increase side effects without improving circadian benefit
-
May desensitize melatonin receptors with chronic use
Clinical observation consistently shows:
-
0.3–1 mg works for circadian alignment
-
Higher doses increase dream vividness, morning grogginess, headache, and sleep fragmentation
Melatonin has a flat dose–response curve for circadian effects.
Immediate-Release vs Prolonged-Release: Not Interchangeable
-
Immediate-release melatonin
-
Best for circadian phase shifting
-
Preferred in delayed sleep phase, jet lag, ADHD
-
-
Prolonged-release melatonin
-
Mimics overnight secretion
-
More useful in elderly patients with fragmented sleep
-
Less effective for phase advancement
-
Using prolonged-release melatonin for circadian delay is a common but avoidable error.
Special Populations: Where Nuance Matters Most
ADHD and Neurodevelopmental Conditions
-
Delayed circadian phase is common
-
Melatonin works best when combined with:
-
Morning bright light exposure
-
Fixed wake-up time
-
-
Late or inconsistent dosing reduces benefit dramatically
Elderly Patients
-
Reduced endogenous melatonin amplitude
-
Increased sensitivity to higher doses
-
Prefer low-dose (0.3–1 mg), early evening dosing
-
Prolonged-release formulations may help sleep maintenance
Depression and Mood Disorders
-
Circadian misalignment is common
-
Melatonin may help phase correction but is not antidepressant
-
Incorrect timing can worsen early morning awakenings
Light Exposure: The Stronger Drug Most People Ignore
Light suppresses melatonin more powerfully than any pill can replace it.
-
Evening screen exposure reduces melatonin secretion
-
Morning light anchors circadian phase
-
Melatonin without light hygiene is often ineffective
Clinically:
You cannot pharmacologically out-supplement poor light behavior.
Safety, Tolerance, and Long-Term Use
Melatonin is generally safe, but not inert.
Potential issues:
-
Next-day sedation
-
Parasomnias at higher doses
-
Interaction with antidepressants, beta-blockers, and alcohol
-
Psychological dependence (“I can’t sleep without it”)
Melatonin should ideally be used as a temporary circadian tool, not a lifelong nightly crutch.
When Melatonin Is Unlikely to Help
Melatonin is not a solution for:
-
Anxiety-driven insomnia
-
Depression-related early morning awakening
-
Untreated sleep apnea
-
Irregular sleep schedules without behavioral change
In these cases, CBT-I, chronotherapy, or treating the primary disorder is more effective.
Clinical Bottom Line
Melatonin is not weak.
It is precise.
Used with biological timing, low doses, and light management, it can gently realign a disrupted circadian system. Used casually at bedtime, it becomes an unreliable sedative with unnecessary side effects.
The difference is not the molecule—it is the model used to prescribe it.
Key Takeaway for Patients and Clinicians
Melatonin works best when treated as circadian medicine, not sleep medicine.
Once that shift in thinking occurs, many “melatonin failures” quietly become successes.
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808