Methylphenidate Dosing & Titration Guide: Children vs Adults, Side Effects, and Comorbidity Management
 Methylphenidate remains a first-line pharmacological treatment for ADHD, yet its clinical effectiveness depends far less on the molecule itself and far more on how it is prescribed, titrated, and monitored.
Methylphenidate remains a first-line pharmacological treatment for ADHD, yet its clinical effectiveness depends far less on the molecule itself and far more on how it is prescribed, titrated, and monitored.
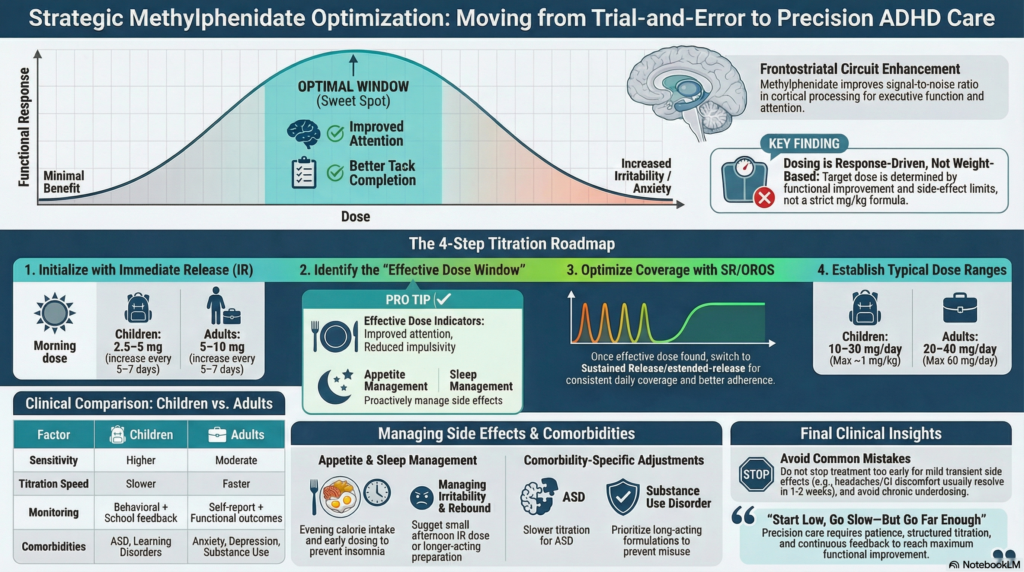
Methylphenidate acts by enhancing dopaminergic and noradrenergic transmission within frontostriatal circuits—networks critical for attention, impulse control, and executive functioning. However, its effects are not linear. Instead, they follow an inverted U-shaped response curve:
- Too little → minimal clinical benefit
- Too much → anxiety, irritability, insomnia
- Optimal dose → improved signal-to-noise ratio in cortical processing
This neurobiological principle explains why methylphenidate dosing is not standardised, but individualised.
Unlike many psychiatric medications, methylphenidate has a rapid onset of action, allowing clinicians to observe meaningful changes within days. While this enables efficient titration, it also introduces complexity: the therapeutic window may be narrow, inter-individual variability is significant, and inadequate titration can lead to either under-treatment or avoidable adverse effects.
Furthermore, the availability of multiple formulations—immediate release, sustained release, and extended-release systems—requires clinicians to align pharmacokinetics with the patient’s daily functional demands, comorbidities, and risk profile.
Thus, prescribing methylphenidate is not a static decision, but a dynamic process of optimisation, integrating:
- Clinical response
- Tolerability
- Functional outcomes
A structured, stepwise approach remains essential to achieving consistent, reproducible, and patient-centred outcomes in ADHD care.
Principles of Dosing: Start Low, Go Slow — But Go Far Enough
Methylphenidate dosing is not weight-based in a strict sense.
Instead, it is:
- Response-driven
- Side-effect limited
The goal is:
✔ Maximum functional improvement
✔ Minimum adverse effects
Children vs Adults: Key Differences
| Factor | Children | Adults |
|---|---|---|
| Sensitivity | Higher | Moderate |
| Starting dose | Lower | Slightly higher |
| Titration speed | Slower | Faster |
| Monitoring | Behaviour + school feedback | Self-report + function |
| Comorbidities | ASD, learning disorders | Anxiety, depression, substance use |
Step-by-Step Titration Strategy
Step 1: Start with Immediate Release (IR)
Children:
- Start: 2.5–5 mg once daily (morning)
- Increase: by 2.5–5 mg every 5–7 days
Adults:
- Start: 5–10 mg once daily
- Increase: by 5–10 mg every 5–7 days
👉 Divide into 2–3 doses if needed
Step 2: Identify the “Effective Dose Window”
Look for:
- Improved attention
- Reduced impulsivity
- Better task completion
Without:
- Irritability
- Appetite suppression
- Sleep disturbance
👉 This is your therapeutic window
Step 3: Optimise Coverage
Once response is established:
- Switch to SR or OROS formulations for:
- School/workday coverage
- Better adherence
- Smoother effect
Step 4: Typical Dose Ranges
Children:
- Usual: 10–30 mg/day
- Max: ~1 mg/kg/day (clinical guidance, not rigid)
Adults:
- Usual: 20–40 mg/day
- Max: up to 60 mg/day (depending on formulation)
Managing Common Side Effects
1. Appetite Suppression
Strategy:
- Encourage high-calorie breakfast before dose
- Shift main calorie intake to evening
- Use nutrient-dense snacks
2. Insomnia
Causes:
- Late dosing
- Excess dose
Management:
- Avoid evening doses
- Reduce afternoon dose
- Consider switching formulation
3. Irritability / Rebound
Clues:
- Evening mood swings
- Sudden drop in effect
Management:
- Add small afternoon IR dose
- Switch to long-acting preparation
- Evaluate for comorbid mood issues
4. Anxiety / Palpitations
Approach:
- Rule out underlying anxiety disorder
- Reduce dose
- Slow titration
- Consider alternative medication if persistent
5. Headache / GI discomfort
Usually transient:
- Hydration
- Dose adjustment
- Often resolves within 1–2 weeks
Comorbidity-Focused Prescribing
ADHD rarely exists in isolation.
1. ADHD + Anxiety
- Start low, titrate slowly
- Treat anxiety if severe first
- Consider combining with:
- Escitalopram
- Propranolol
2. ADHD + Depression
- Treat both conditions
- Combination approach often needed:
- Bupropion (dual benefit)
- SSRIs if mood dominant
3. ADHD + Substance Use
- Prefer long-acting formulations
- Avoid misuse-prone IR dosing
- Close monitoring essential
4. ADHD + Autism Spectrum Disorder
- Higher sensitivity to side effects
- Slower titration
- Lower optimal doses
5. ADHD + Sleep Disorders
- Correct sleep hygiene first
- Avoid late dosing
- Evaluate circadian rhythm issues
When Methylphenidate Doesn’t Work
Consider:
- Incorrect diagnosis
- Suboptimal dose
- Poor adherence
- Comorbidities masking response
Alternatives include:
- Atomoxetine
- Guanfacine
Monitoring Checklist
- Weight (especially in children)
- Appetite
- Sleep
- Blood pressure / pulse
- Academic / occupational functioning
- Behavioural feedback
Key Clinical Insight
The most common mistake is:
👉 Stopping too early due to mild side effects
The second most common:
👉 Underdosing
Optimal treatment requires:
- Patience
- Structured titration
- Continuous feedback
Conclusion
Methylphenidate is highly effective — but only when used strategically.
- Start low
- Titrate methodically
- Treat comorbidities
- Monitor function, not just symptoms
This transforms ADHD treatment from:
❌ Trial-and-error
to
✔ Precision-based care
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
With expertise in ADHD assessment using QEEG and CPT, and structured pharmacological strategies, Dr. Srinivas focuses on accurate diagnosis and personalised treatment in real-world clinical settings.