Obsessive Images: When the Mind Attacks With Pictures
Understanding intrusive mental imagery in OCD
When people think of Obsessive–Compulsive Disorder (OCD), they usually imagine repetitive thoughts or compulsive behaviors. Far less discussed—but often far more disturbing—are obsessive images: vivid, unwanted mental pictures that intrude into consciousness without warning.
Patients often say, “It’s not a thought… it’s like a scene playing in my head.”
And that distinction matters.
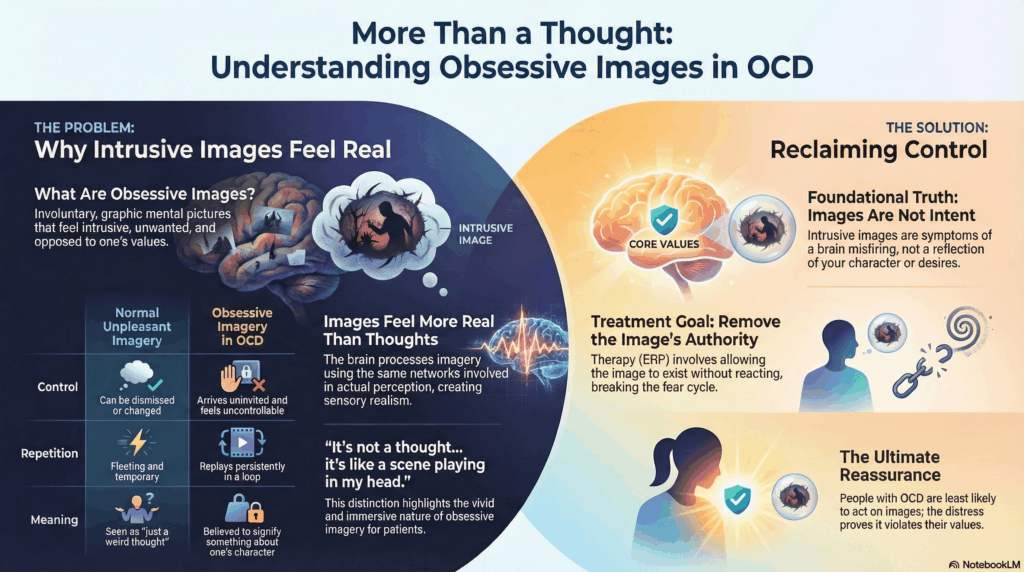
What Are Obsessive Images?
Obsessive images are intrusive mental pictures that appear involuntarily and repeatedly. They are:
-
Graphic and emotionally charged
-
Experienced as intrusive, not imagined on purpose
-
Distressing, ego-dystonic, and unwanted
-
Often resistant to reassurance
Common themes include:
-
Violent images (harming loved ones, accidents, death)
-
Sexual images (often taboo or morally distressing)
-
Contamination imagery (germs spreading, bodily decay)
-
Religious or blasphemous imagery
-
Catastrophic “flash-forward” scenes
These images are not fantasies, desires, or intentions. They are symptoms.
Why Images Feel Worse Than Thoughts
Images carry sensory realism. The brain processes imagery using many of the same networks involved in real perception. As a result:
-
Images feel more real than verbal thoughts
-
Emotional response is stronger and faster
-
Patients fear loss of control or moral corruption
-
Thought–action fusion becomes more intense
A patient may know logically, “I won’t do this,” but emotionally, the image says, “This is happening.”
That mismatch fuels panic.
Obsessive Images vs Normal Mental Imagery
Most people can imagine unpleasant scenes briefly. The difference in OCD lies in:
-
Lack of control: the image arrives uninvited
-
Repetition: the same image replays again and again
-
Meaning attribution: “Why would my brain show this unless it means something?”
-
Compulsive responses: mental neutralising, avoidance, reassurance, checking
The distress comes not from the image itself—but from what the person believes the image says about them.
The Cognitive Mechanism Behind Obsessive Images
Obsessive images arise from the same mechanisms as obsessive thoughts, but with added intensity:
-
Hyperactive threat detection
-
Overactive error-monitoring systems
-
Inflated responsibility and moral sensitivity
-
Poor tolerance of uncertainty
-
Difficulty disengaging attention from internal stimuli
The brain treats imagery as evidence, not imagination.
Common Compulsions Linked to Obsessive Images
Unlike visible rituals, these are often covert:
-
Mental neutralising (“canceling” the image)
-
Replacing the image with a “good” image
-
Praying repeatedly
-
Avoiding triggers (people, places, objects)
-
Seeking reassurance (“Would I ever do this?”)
-
Suppressing thoughts (which paradoxically strengthens them)
Because these rituals are internal, obsessive images are frequently missed or misdiagnosed.
Treatment Principles: What Actually Helps
1. Psychoeducation Is Therapeutic
Patients must understand:
-
Images ≠ intent
-
Images ≠ desire
-
Images ≠ prediction
Intrusive imagery reflects brain misfiring, not character.
2. ERP Works—But Must Be Image-Focused
Exposure involves:
-
Allowing the image to arise
-
Resisting neutralisation
-
Staying with discomfort
-
Letting anxiety rise and fall naturally
The goal is not to erase images, but to remove their authority.
3. Stop Fighting the Image
Suppression strengthens imagery. Learning to observe the image as a mental event—without judgment or action—is key.
4. Medication Often Plays a Supportive Role
SSRIs reduce:
-
Image intensity
-
Emotional charge
-
Sense of urgency
This creates space for therapy to work.
5. Insight Grows After Experience, Not Explanation
Patients rarely believe reassurances initially. Insight emerges when repeated exposure proves:
“The image can exist—and nothing happens.”
A Crucial Reassurance
People with OCD are least likely to act on intrusive images. The distress they feel is precisely because the image violates their values.
The mind produces noise. OCD convinces the person that the noise is a warning.
Treatment teaches the brain to stop listening to false alarms.
Closing Perspective
Obsessive images are one of the most frightening experiences in psychiatry—not because they signal danger, but because they masquerade as it.
Recovery begins when patients learn:
-
Thoughts and images are events, not truths
-
The brain can misfire without meaning
-
Control is regained by allowing, not fighting
This is not passive acceptance. It is neuropsychological retraining.
About the Author
Dr. Srinivas Rajkumar T
MD (AIIMS, New Delhi), DNB Psychiatry, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Dr. Srinivas Rajkumar T has extensive experience in treating OCD, including intrusive thoughts, obsessive images, poor-insight OCD, and treatment-resistant cases. His approach integrates evidence-based psychotherapy (ERP-informed), pharmacological optimisation, and neuroscience-guided tools where appropriate.
He practices at Apollo Clinic Velachery (Opp. Phoenix Mall), Chennai, and offers both in-person and online consultations.
📧 srinivasaiims@gmail.com
📞 +91-8595155808
This article is part of an ongoing series on OCD, cognition, and modern psychiatric care.