Stopping Escitalopram (Nexito): A Nuanced, Evidence-Informed Patient Guide
 Antidepressants are not meant to be lifelong medications for everyone. This is a point often missed in public discussions and sometimes even in clinical conversations. Major international guidelines—including those from the National Institute for Health and Care Excellence (NICE) and the American Psychiatric Association (APA)—recommend that antidepressants be used for a time-limited period, tailored to the individual’s diagnosis, severity, and risk of relapse.
Antidepressants are not meant to be lifelong medications for everyone. This is a point often missed in public discussions and sometimes even in clinical conversations. Major international guidelines—including those from the National Institute for Health and Care Excellence (NICE) and the American Psychiatric Association (APA)—recommend that antidepressants be used for a time-limited period, tailored to the individual’s diagnosis, severity, and risk of relapse.
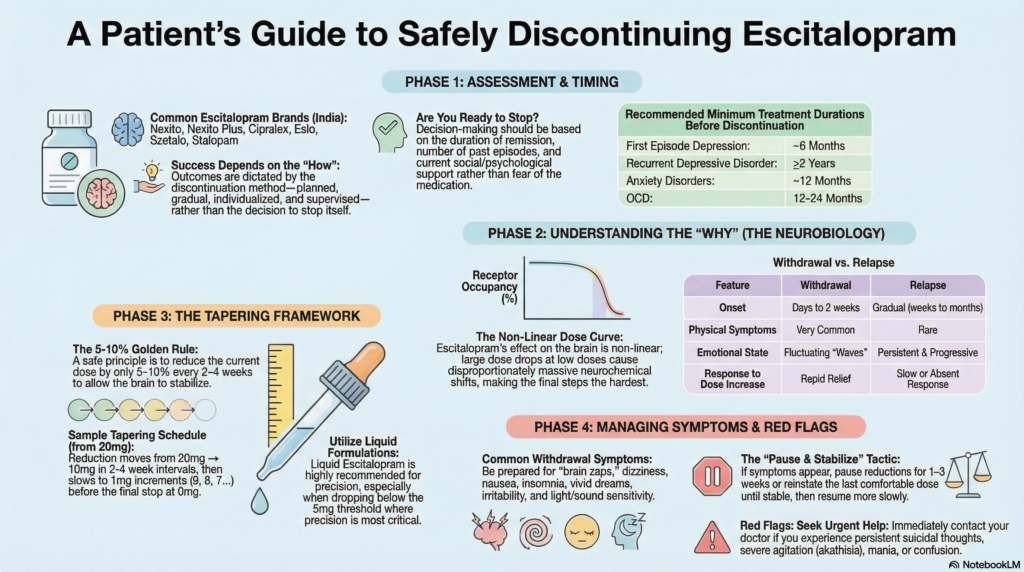
For most people with a first episode of depression, guidelines suggest continuing antidepressant treatment for about 6 months after full recovery. For individuals with recurrent depressive disorder, longer maintenance—often 2 years or more—may be appropriate. Similar principles apply to anxiety disorders and obsessive–compulsive disorder (OCD), where medications are usually continued for at least 12 months after stable improvement, not indefinitely.
Escitalopram—commonly prescribed in India under the brand name Nexito—is widely used for depression, anxiety disorders, panic disorder, social anxiety, and OCD. For many patients, it is an essential part of recovery. For others, a point comes where stopping the medication becomes a reasonable and evidence-based consideration.
Stopping escitalopram is possible for many people, but outcomes depend far more on how discontinuation is done than on the decision itself.
This article offers a balanced, practical, and evidence-informed guide to stopping escitalopram safely—grounded in neurobiology, clinical guidelines, and real-world patient experience.
What Is Escitalopram? (Common Brand Names in India)
Escitalopram is a Selective Serotonin Reuptake Inhibitor (SSRI) commonly prescribed for:
-
Major Depressive Disorder
-
Generalised Anxiety Disorder
-
Panic Disorder
-
Social Anxiety Disorder
-
Obsessive–Compulsive Disorder (OCD)
Common Indian Brand Names of Escitalopram
Escitalopram is available in India under several brand names, including:
-
Nexito / Nexito Plus
-
Cipralex
-
Eslo
-
Szetalo
-
Stalopam
-
Esertia
-
Escita
-
Elopram
-
Depranex
All contain the same active molecule. The principles of tapering and withdrawal apply equally, regardless of brand.
Is It Safe to Stop Escitalopram?
Yes—for many patients, escitalopram can be stopped safely.
However, discontinuation should be:
-
Planned
-
Gradual
-
Individualised
-
Supervised
The brain adapts to antidepressants over time. Abrupt or rapid stopping can overwhelm this adaptation, leading to withdrawal symptoms, which are frequently mistaken for relapse.
Before You Stop Escitalopram: Is This the Right Time?
The decision to discontinue escitalopram should be based on clinical context, not impatience or fear of medication.
Key factors include:
-
Duration of remission
-
Number and severity of past episodes
-
Presence of ongoing stressors
-
Psychological and social supports
-
Personal preference
Typical Maintenance Durations (Guideline-Informed)
| Condition | Usual minimum continuation after recovery |
|---|---|
| First episode depression | ~6 months |
| Recurrent depressive disorder | ≥2 years |
| Anxiety disorders | ~12 months |
| OCD | Often 12–24 months |
| Severe or suicidal depression | Longer-term, individualised |
These are guideline-based averages, not fixed rules.
Withdrawal vs Relapse: Understanding the Difference
One of the most common fears during tapering is mistaking withdrawal symptoms for illness recurrence.
| Feature | Withdrawal | Relapse |
|---|---|---|
| Onset | Days to 1–2 weeks after dose change | Gradual over weeks–months |
| Physical symptoms | Common | Rare |
| Emotional symptoms | Fluctuating | Persistent |
| Response to dose increase | Rapid | Slow or absent |
| Pattern | Waves and windows | Progressive worsening |
Escitalopram is considered a moderate-risk SSRI for withdrawal, but difficulties can still occur—especially with fast tapers.
Why Slow Tapering Matters (Especially at Low Doses)
Escitalopram’s effect on serotonin transporters follows a non-linear dose–response curve.
This means:
-
Large dose drops at low doses cause disproportionately large neurochemical shifts
-
The final steps of tapering are often the hardest
This is neurobiology, not dependence or weakness.
How to Stop Escitalopram Safely: A Practical Framework
A commonly safe principle is:
Reduce by 5–10% of the current dose every 2–4 weeks
For long-term users or sensitive individuals:
-
5% reductions per month
-
Longer holding periods
-
Very small final dose steps
Example Escitalopram Taper Schedule (Starting at 20 mg)
| Dose (mg) | Interval |
|---|---|
| 20 | Baseline |
| 18 → 16 → 14 → 12 → 10 | 2–4 weeks each |
| 9 → 8 → 7 → 6 → 5 | 2–4 weeks each |
| 4 → 3 → 2 → 1 | 3–4 weeks each |
| 0 | Stop |
Liquid escitalopram allows precise dose reductions, especially below 5 mg.
Common Escitalopram Withdrawal Symptoms
-
Brain zaps, dizziness
-
Nausea, loose stools
-
Insomnia, vivid dreams
-
Anxiety, irritability
-
Brain fog, concentration difficulty
-
Light or sound sensitivity
Symptoms usually occur in waves, not a steady decline.
Risk Factors for Difficult Withdrawal
-
Long duration of treatment
-
Higher doses
-
Previous withdrawal problems
-
Rapid past tapers
-
High baseline anxiety
What to Do If Withdrawal Symptoms Appear
-
Pause further reductions
-
Allow 1–3 weeks for stabilisation
-
Reinstate the last comfortable dose if needed
-
Resume tapering more slowly
Most prolonged difficulties resolve with this approach.
When Long-Term Treatment May Be Appropriate
Long-term escitalopram use may be appropriate in:
-
Multiple severe depressive episodes
-
Recurrent suicidal depression
-
Chronic anxiety with repeated relapse
-
Bipolar spectrum conditions (with caution)
Stopping medication is not a moral goal—well-being is.
Psychological Factors During Tapering
Heightened self-monitoring and fear of relapse are common.
Supportive psychotherapy helps differentiate withdrawal from recurrence and improves confidence.
Red Flags Requiring Urgent Medical Review
-
Persistent suicidal thoughts
-
Severe agitation or akathisia
-
Manic symptoms
-
Confusion or neurological changes
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist
Dr. Srinivas Rajkumar T is a Chennai-based psychiatrist with extensive experience in mood and anxiety disorders, long-term psychopharmacology, and safe antidepressant tapering. His approach integrates international guidelines, neurobiological understanding, and patient-centred care.
📍 Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com
📞 +91-8595155808
This article is for educational purposes and does not replace personalised medical advice. Medication changes should always be undertaken under psychiatric supervision.