🧠 Seizure vs Pseudoseizure (PNES): A Detailed Clinical Approach
 Distinguishing epileptic seizures from psychogenic non-epileptic seizures in real-world practice
Distinguishing epileptic seizures from psychogenic non-epileptic seizures in real-world practice
The differentiation between epileptic seizures and psychogenic non-epileptic seizures (PNES) remains one of the most clinically challenging tasks in neurology and psychiatry. Misdiagnosis is common, often leading to years of inappropriate anti-epileptic treatment, persistent disability, and significant psychosocial burden.
PNES is best conceptualized under:
- Functional Neurological Symptom Disorder
- Dissociative Neurological Symptom Disorder
These are involuntary conditions, not consciously produced behaviors.
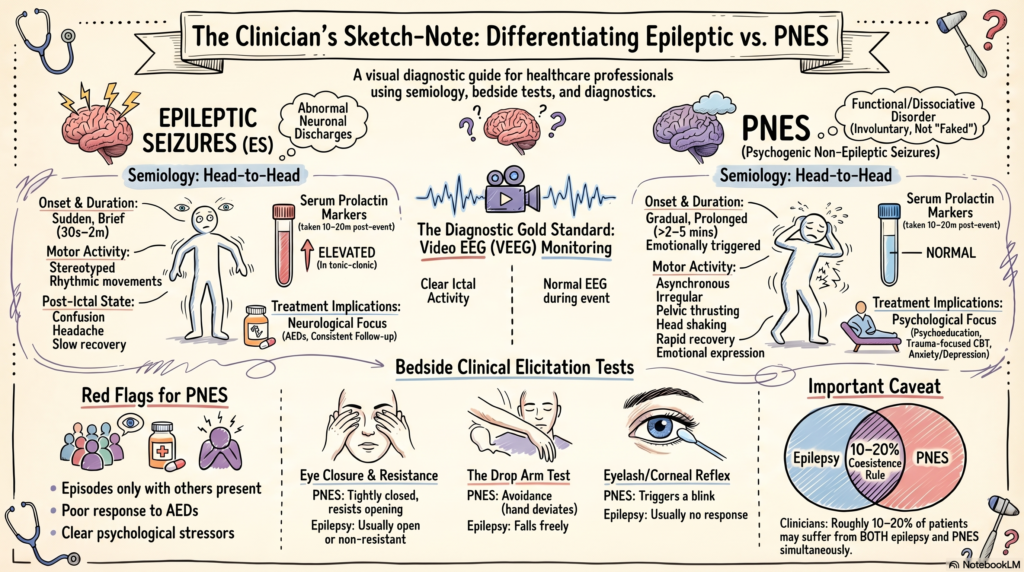
🔍 1. The Gold Standard: Video EEG Monitoring
Why it matters
The only definitive way to differentiate is:
👉 Simultaneous video + EEG recording during an event
Interpretation
- Epileptic seizure: Clear ictal epileptiform activity
- PNES: Normal EEG during apparent seizure
Clinical nuance
- Some frontal lobe seizures may have subtle EEG changes → interpret cautiously
- Always correlate clinical semiology + EEG
🧪 2. Bedside Clinical Elicitation Tests
These are supportive tools, not diagnostic in isolation.
🔹 Eye Closure & Resistance
- Epilepsy: Eyes usually open or non-resistant
- PNES: Eyes tightly closed, active resistance to opening
👉 Suggests preserved voluntary control
🔹 Eyelash / Corneal Reflex
- Lightly touch eyelashes
- Epilepsy: No blink during generalized seizure
- PNES: Blink or avoidance
🔹 Drop Arm Test
- Lift arm and drop over face
- Epilepsy: Falls freely (may hit face)
- PNES: Avoidance → hand deviates
👉 Indicates protective motor control
🔹 Pain Response
- Nail bed pressure / trapezius squeeze
- Epilepsy: No purposeful response
- PNES: Withdrawal or organized reaction
🔹 Suggestibility / Interruption
- Calm verbal suggestion or distraction
- PNES: Episode may reduce or stop
- Epilepsy: No interruption
⚠️ Use ethically; avoid deception
⚡ 3. Semiology: Pattern Recognition
This is where clinical expertise becomes critical.
🔹 Onset
- Epilepsy: Sudden
- PNES: Gradual, often emotionally triggered
🔹 Motor Activity
- Epilepsy: Stereotyped, rhythmic, synchronous
- PNES: Asynchronous, irregular, variable
🔹 Duration
- Epilepsy: Typically 30 sec – 2 min
- PNES: Often prolonged (>2–5 min), fluctuating
🔹 Characteristic Movements
- Pelvic thrusting: More common in PNES
- Side-to-side head shaking: Suggestive of PNES
- Opisthotonus-like postures: May be seen in PNES
🔹 Tongue Bite
- Epilepsy: Lateral border
- PNES: Tip of tongue (if present)
🔹 Incontinence
- Epilepsy: Common
- PNES: Rare
🔹 Post-Ictal State
- Epilepsy: Confusion, drowsiness, headache
- PNES: Rapid recovery, emotional expression
🧪 4. Laboratory Markers (Adjuncts Only)
🔹 Serum Prolactin (10–20 min post-event)
- Elevated in:
- Generalized tonic-clonic seizures
- Complex partial seizures
- Usually normal in PNES
⚠️ Limitations:
- Not useful for absence seizures
- False positives/negatives occur
🔹 Creatine Kinase (CK)
- May rise after true seizures due to muscle breakdown
- Typically normal in PNES
🧠 5. Key Clinical Red Flags for PNES
- Long, dramatic, fluctuating episodes
- Occur in presence of others
- Eyes tightly closed
- Preserved awareness intermittently
- Poor response to anti-epileptic drugs
- Clear psychological stressors
⚠️ 6. Critical Clinical Caveats
🔸 Coexistence
- 10–20% patients may have both epilepsy and PNES
🔸 Avoid premature labeling
- Mislabeling as “fake” → therapeutic rupture
🔸 Always rule out:
- Frontal lobe epilepsy
- Syncope
- Movement disorders
🧩 7. Integrative Understanding
| Domain | Epileptic Seizure | PNES |
|---|---|---|
| Pathophysiology | Abnormal neuronal discharge | Functional/dissociative mechanism |
| EEG | Abnormal | Normal |
| Control | Involuntary | Involuntary (but psychogenic) |
| Treatment | Anti-epileptics | Psychotherapy |
🛠️ 8. Treatment Implications
Epilepsy
- Anti-epileptic drugs
- Neurological follow-up
PNES
- Psychoeducation (crucial first step)
- Trauma-focused therapy / CBT
- Address comorbid depression, anxiety
👉 Early correct diagnosis significantly improves outcomes
📌 One-Line Clinical Wisdom
👉 “EEG confirms, but semiology guides suspicion.”
✍️ About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
At the Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall), I routinely evaluate complex presentations including dissociative disorders, PNES, ADHD, and cognitive disorders using a combination of:
- Detailed clinical assessment
- Objective tools (including neurocognitive testing and QEEG where indicated)
- Evidence-based, individualized treatment planning
If you or your patient is struggling with unclear seizure-like episodes or treatment-resistant symptoms, a structured evaluation can help arrive at the right diagnosis and avoid years of unnecessary treatment.
✉ srinivasaiims@gmail.com 📞 +91-8595155808