Delusions in Psychiatry: From Disturbance of Meaning to Therapeutic Understanding
 Introduction: Moving Beyond “False Belief”
Introduction: Moving Beyond “False Belief”
Delusions are often introduced as false, fixed beliefs. While convenient, this definition is fundamentally inadequate.
As emphasized in classical psychopathology:
“It would be a superficial and wrong answer… to call a delusion a false belief which is held with incorrigible certainty.”
This is not merely a semantic correction—it reflects a deeper truth:
Delusions are disturbances in the experience of reality, not just errors in belief.
Understanding this distinction is essential—not only for diagnosis, but for meaningful therapeutic engagement.
The Classical Framework—and Its Limitations
Karl Jaspers described delusions as:
“Held with extraordinary conviction… impervious to counter-argument… content is impossible.”
Yet even he cautioned:
“To say simply that a delusion is a mistaken idea… gives only a superficial and incorrect answer.”
Why does this definition fail?
Because:
- Conviction alone is not pathological
- Cultural beliefs may appear irrational but are shared
- Even true events can be held delusionally
As the text insightfully notes:
“There is no delusional idea… which cannot be exceeded in its absurdity by the conviction of fanatics.”
👉 Therefore:
- Falsity ≠ delusion
- Conviction ≠ delusion
The Phenomenological Turn: Form Over Content
Drawing from Immanuel Kant, Jaspers introduced a crucial distinction:
- Content (Inhalt) → what is believed
- Form (Form) → how it is experienced
Your source emphasizes:
“Phenomenology… does not teach us anything about the contents… but about the forms.”
Clinical Implication:
Two patients may say:
- “People are watching me”
But:
- One → anxious suspicion
- One → delusional certainty
👉 The form of experience defines pathology.
German Psychopathological Concepts: Precision in Understanding
The German tradition offers conceptual clarity that is indispensable.
1. Wahn (Delusion)
- A disturbance in belief
- But more importantly: a disturbance in experience
2. Primäre Wahnerlebnis (Primary Delusional Experience)
“Phenomenologically it is an experience.”
This is the core of delusion:
- Not derived from reasoning
- Not an interpretation
- A direct transformation of reality experience
3. Unmittelbar (Unmediated)
“The primary delusion is a direct, unmediated phenomenon.”
- Immediate
- Not processed through thought
- Experienced as self-evident
4. Gedanklich vermittelt (Thought-mediated)
- Applies to:
- Normal beliefs
- Overvalued ideas
- Secondary delusions
👉 These involve reflection and interpretation
5. Verstehen vs Nicht-Verstehen
- Verstehbar (understandable) → psychologically traceable
- Nicht verstehbar (un-understandable) → cannot be derived
👉 Primary delusions are:
Nicht verstehbar
Primary vs Secondary Delusions: The Core Distinction
Primary Delusions (True Delusions)
“Psychologically irreducible… something final.”
Characteristics:
- Sudden
- Not derived from prior experience
- Not psychologically explainable
👉 Represent a break in reality
Secondary (Delusion-like) Ideas
“Emerge understandably from preceding affects… or experiences.”
Examples:
- Depression → guilt delusions
- Mania → grandiosity
👉 These are extensions of emotional states, not primary delusions
Delusion as Disturbance of Meaning (Bedeutung)
This is the most important conceptual insight.
Jaspers states:
“Perceptions are never mechanical… there is always a perception of meaning.”
In delusion:
“The awareness of meaning undergoes a radical transformation.”
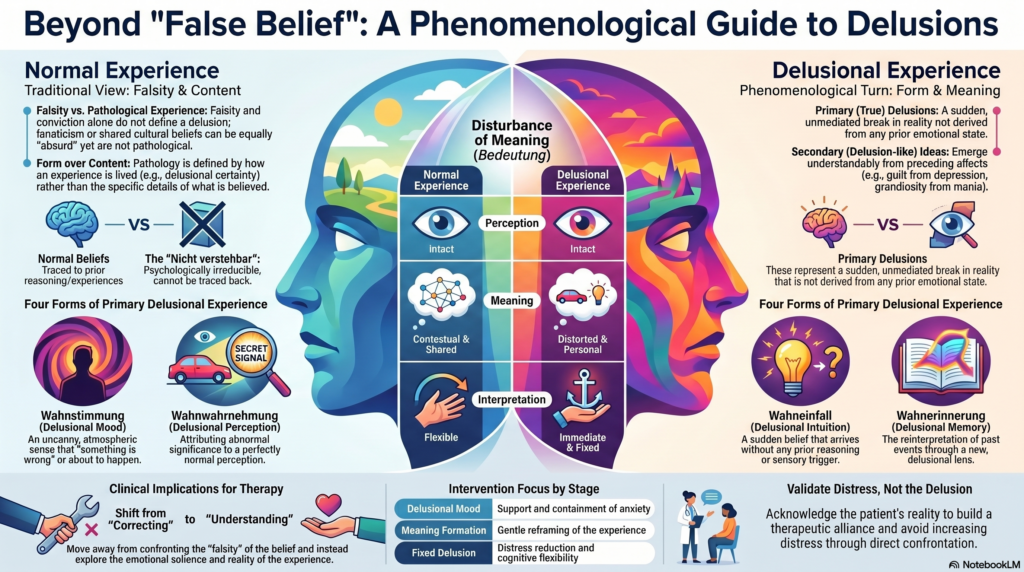
What Actually Changes?
| Component | Normal Experience | Delusion |
|---|---|---|
| Perception | Intact | Intact |
| Meaning | Contextual | Distorted |
| Interpretation | Flexible | Immediate & fixed |
👉 The world is not misperceived
👉 It is mis-signified
Forms of Primary Delusional Experience
1. Wahnstimmung (Delusional Mood / Trema)
- Uncanny atmosphere
- Sense that “something is wrong”
2. Wahnwahrnehmung (Delusional Perception)
“Abnormal significance… attributed to normal perception.”
3. Wahneinfall (Delusional Intuition)
- Sudden belief
- No reasoning
4. Wahnerinnerung (Delusional Memory)
- Past reinterpreted
How Do Delusions Form? (Integrated Models)
Delusions are best understood through a multifactorial lens.
1. Perceptual-Cognitive Model (Maher)
- Abnormal perception → search for meaning → delusion
2. Dopamine / Salience Model
- Irrelevant stimuli gain significance
“Many perceptions… gain high personal significance.”
3. Cognitive Bias Models
- Jumping to conclusions
- Attribution bias
- Theory of mind deficits
4. Psychodynamic Model
- Projection of internal conflict
5. Stress–Vulnerability Model
Stress + vulnerability → anomalous experience → meaning-making → delusion
Why Delusions Persist
Delusions are maintained by:
“Need for consistency… poverty of interpersonal communication… reinforcement by behavior.”
They also:
- Reduce uncertainty
- Provide coherence
- Protect self-esteem
Clinical Implications: From Theory to Practice
1. Shift in Clinical Thinking
From:
- “This belief is false”
To:
- “This reality is experienced differently”
2. Therapeutic Stance
- Avoid confrontation
- Validate distress
- Explore experience
3. Working at the Level of Meaning
Instead of challenging:
- Facts
Work with:
- Meaning
- Emotional salience
- Context
4. Timing Matters
| Stage | Intervention Focus |
|---|---|
| Delusional mood | Support, containment |
| Meaning formation | Gentle reframing |
| Fixed delusion | Distress reduction, flexibility |
A Deeper Clinical Insight
Delusions are not random errors.
They are:
Attempts to make sense of an altered experiential world
Removing them without understanding:
- Increases distress
- Weakens alliance
Working with them:
- Builds trust
- Enables gradual restructuring
Final Conceptual Synthesis
Delusion is a disturbance of meaning, experienced immediately (unmittelbar), arising in an un-understandable (nicht verstehbar) manner, and lived as reality rather than inferred as belief.
Take-Home Message
When evaluating a patient, ask:
- Is this belief derived or immediate?
- Is it understandable or not?
- Is it a judgment or an experience?
Because:
Delusions are not simply beliefs to be corrected—they are realities to be understood and carefully reconstructed.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808