Predictive Coding and Psychosis: When the Brain’s Prediction System Goes Wrong
 Schizophrenia is often described through its most visible symptoms: hallucinations, delusions, disorganized thinking, negative symptoms and impaired functioning. However, these symptoms are only the surface of a much deeper disturbance. Modern computational psychiatry is increasingly asking a more fundamental question:
Schizophrenia is often described through its most visible symptoms: hallucinations, delusions, disorganized thinking, negative symptoms and impaired functioning. However, these symptoms are only the surface of a much deeper disturbance. Modern computational psychiatry is increasingly asking a more fundamental question:
How does the brain decide what is real?
One of the most influential answers comes from the theory of predictive coding. This model suggests that the brain is not a passive camera recording the world. Instead, it is an active prediction machine. It constantly predicts what is likely to happen next, compares those predictions with incoming sensory information, and updates its understanding of reality based on the mismatch.
In simple terms, the brain is always asking:
“Is this what I expected?”
“Should I trust my expectation?”
“Should I trust this new sensory signal?”
“Does this event mean something important?”
In psychosis, this prediction system may become unstable. The person may begin to assign too much significance to ordinary events, experience internally generated thoughts as external, or form strong beliefs that resist correction despite contrary evidence. Predictive coding offers a powerful framework to connect neurobiology, psychology and subjective experience in schizophrenia.
The Brain as a Prediction Machine
In everyday life, perception feels immediate. We open our eyes and assume we are simply seeing the world as it is. But the brain does much more than receive information. It interprets sensory signals based on prior experience.
For example, when we hear footsteps behind us in a familiar hospital corridor, we do not analyze every sound wave. The brain rapidly predicts: “This is probably a colleague walking.” If the footsteps are unusually fast, heavy or close, a prediction error is generated: “Something is different.” The brain then updates its interpretation.
Predictive coding uses a few key concepts:
Prior means what the brain expects based on past experience.
Sensory input means the information currently coming from the senses.
Prediction error means the mismatch between what was expected and what actually occurred.
Precision means how much confidence the brain gives to a signal.
Precision is crucial. A signal can be noisy but still feel important if the brain gives it high precision. Conversely, a meaningful signal may be ignored if the brain gives it low precision.
This is where psychosis may begin: not necessarily with a false belief, but with a disturbance in how the brain weighs evidence.
What Happens in Psychosis?
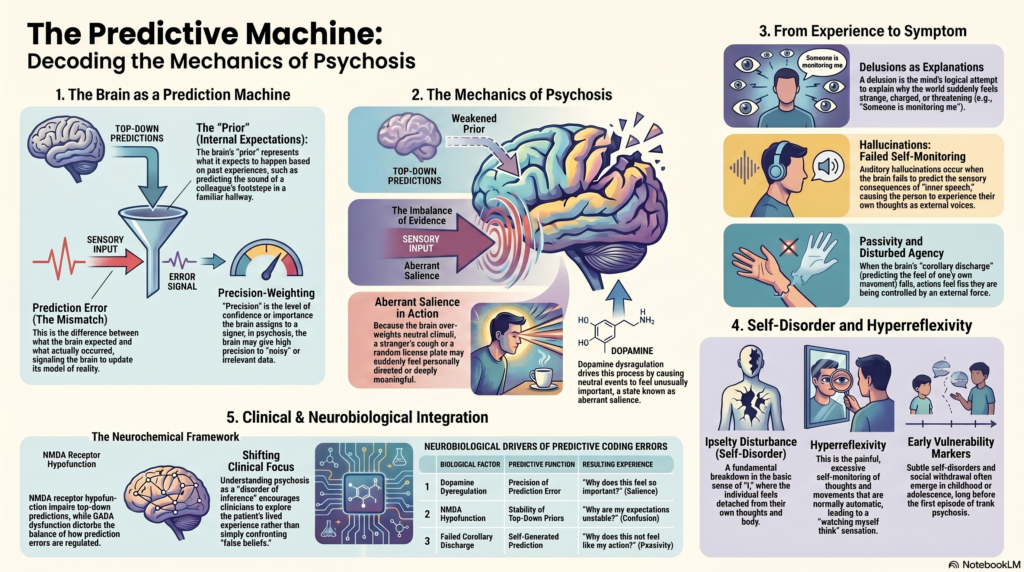
The classical predictive coding account proposes that psychosis involves an imbalance between prior expectations and sensory information. Specifically, prior beliefs may become less precise, while incoming sensory signals or prediction errors may be given excessive precision. As a result, the person’s brain becomes overly driven by moment-to-moment sensory events.
Ordinary experiences begin to feel unusual.
A stranger coughing may feel personally directed.
A number plate may seem like a hidden code.
A newsreader’s pause may feel like a message.
A passing glance may feel threatening.
A random coincidence may feel deeply meaningful.
This does not mean the person is “making things up.” From the person’s internal experience, the world has genuinely changed. The brain is assigning abnormal significance to events that others would dismiss as irrelevant.
This is closely related to aberrant salience, a model proposed by Shitij Kapur. In aberrant salience, dopamine dysregulation causes neutral stimuli to feel unusually important. Predictive coding extends this idea by explaining how abnormal salience can arise from disturbed prediction errors and altered precision-weighting.
Delusions: The Mind Trying to Explain Abnormal Experience
A delusion is often described as a fixed false belief. But clinically, that definition is incomplete. It does not explain how the belief forms.
Predictive coding gives us a more humane and mechanistic explanation.
First, the person experiences abnormal prediction errors.
The world feels strange, significant, threatening or personally charged.
Then the mind tries to explain why this is happening.
A delusional belief emerges as an explanation for the altered experience.
For example:
“People are looking at me differently.”
“The TV seems to be referring to me.”
“There must be a system behind this.”
“Someone is monitoring me.”
The belief may initially be tentative, but over time it can become more fixed. The paper highlights an important paradox: early psychosis may involve weak priors and excessive prediction errors, but chronic delusions may involve overly strong high-level beliefs that resist updating.
This is clinically important. It suggests that delusions may evolve across time.
In early phases, the patient may be confused, perplexed and searching for meaning. In later phases, the delusional explanation may become consolidated. Once the belief becomes a strong high-level prior, new information may be interpreted through that belief. Contradictory evidence may no longer weaken the delusion; it may even be absorbed into it.
This explains why arguing directly against a delusion often fails. The problem is not simply lack of logic. The person’s entire prediction system may be organized around a different model of reality.
Hallucinations: When Perception Is Overpowered by Prediction
Hallucinations are also well explained by predictive coding, but the mechanism is complex.
One model suggests that hallucinations occur when internally generated signals are not properly recognized as self-generated. For example, inner speech may not be tagged correctly as one’s own thought. It may then be experienced as an external voice.
This overlaps with the concept of corollary discharge.
Normally, when we speak, move or think, the brain predicts the sensory consequences of our own actions. Because the brain expects these consequences, they feel self-generated. But if this predictive signal is weak, one’s own inner speech may feel surprising or external.
This can help explain auditory hallucinations such as hearing voices.
However, the predictive coding literature also suggests another mechanism: hallucinations may involve overly strong top-down priors. If the brain strongly expects speech, it may impose speech-like perception onto ambiguous sound. This is similar to seeing faces in clouds, but in the auditory domain.
So hallucinations may involve both:
- Failure to recognize self-generated inner speech.
- Excessive top-down expectation of speech.
- Abnormal precision given to internally generated signals.
- Disturbed agency and self-monitoring.
This explains why the experience of voices can feel so real. The percept is not imaginary in the ordinary sense. The brain’s inference system has generated a perceptual experience that carries the force of reality.
Passivity Phenomena: “My Actions Are Not Mine”
Some of the most characteristic symptoms of schizophrenia involve disturbed agency.
Patients may report:
“My thoughts are being inserted.”
“My actions are controlled by someone else.”
“My body is being moved.”
“My thoughts are being broadcast.”
“Someone is influencing my mind.”
These are sometimes called passivity phenomena or first-rank symptoms.
Predictive coding explains these symptoms through disturbed self-monitoring. In this framework, corollary discharge becomes a prediction about the sensory consequences of one’s own action. If the prediction fails, the action or thought becomes surprising. The brain may then infer that it came from outside.
A simple example:
Normally:
“I intend to move my hand.”
“My brain predicts the movement.”
“The hand moves as expected.”
“This action feels like mine.”
In schizophrenia-spectrum psychosis:
“I intend to move.”
“The predictive signal is weak.”
“The movement feels unexpected.”
“The brain infers external control.”
This mechanism links predictive coding with self-disorder. The problem is not only abnormal perception. It is abnormal ownership of experience.
Self-Disorder: The Deeper Layer Beneath Psychosis
Recent phenomenological psychiatry has emphasized that schizophrenia is not only a disorder of beliefs or perceptions. It may involve a disturbance in the basic sense of self.
This is called Self-Disorder or Ipseity Disturbance.
Self-disorder refers to subtle disturbances in the most basic sense that “I am the subject of my experiences.” It may involve feeling detached from one’s thoughts, lacking a natural sense of presence, feeling alienated from one’s body, or experiencing the world as strangely unreal.
The 2025 Schizophrenia Bulletin paper on ipseity argues that self-disorders are not merely late consequences of psychosis. They may emerge in childhood or adolescence and may represent an early vulnerability marker for schizophrenia-spectrum conditions.
This is where predictive coding and phenomenology meet.
If the brain cannot reliably predict the consequences of its own actions, thoughts and bodily states, then the basic sense of agency may weaken. If agency weakens, thoughts may feel less “mine.” If thoughts feel less mine, the person may become hyperaware of inner experience. This can lead to hyperreflexivity — a painful, excessive self-monitoring of processes that are normally automatic.
In ordinary life, we do not constantly examine whether our thoughts belong to us. In self-disorder, this automatic ownership becomes unstable.
Hyperreflexivity: When the Mind Turns on Itself
Hyperreflexivity is a central concept in the ipseity model of schizophrenia.
It refers to a condition where normally automatic aspects of experience become objects of intense attention. The person may become painfully aware of their own thoughts, bodily sensations, gaze, speech, posture or intentions.
For example:
“I am watching myself think.”
“My thoughts feel like objects.”
“I cannot act naturally.”
“I feel detached from my own body.”
“I am too aware of my own awareness.”
This is not ordinary overthinking. It is a structural change in consciousness.
Predictive coding may help explain why this occurs. If the brain’s automatic predictions about self-generated experience become unreliable, then the person may have to consciously monitor what should normally remain implicit. Automatic selfhood becomes effortful self-observation.
This can be exhausting. It may contribute to social withdrawal, anxiety, perplexity and loss of spontaneity.
The Developmental Perspective
A major strength of the newer self-disorder literature is its developmental perspective.
Schizophrenia does not suddenly appear from nowhere in early adulthood. Many individuals show subtle developmental vulnerabilities long before psychosis: social oddness, anxiety, unusual perceptual experiences, motor abnormalities, cognitive changes, emotional withdrawal or a feeling of being fundamentally different.
The ipseity paper argues that self-disorder may begin as an early alteration in minimal selfhood, which becomes more visible when the adolescent develops greater reflective awareness. In other words, adolescence may not be the beginning of the disturbance; it may be the stage at which the person becomes able to notice and describe it.
This has clinical implications.
When a young person presents with social withdrawal, unusual perceptual experiences, intense existential concerns, suspiciousness or odd self-descriptions, the clinician should not only ask, “Are there hallucinations or delusions?” We must also ask:
“Has the person’s basic sense of self changed?”
“Do thoughts feel like their own?”
“Does the body feel inhabited?”
“Does the world feel natural or staged?”
“Is the person losing effortless immersion in social reality?”
These questions may reveal early schizophrenia-spectrum vulnerability before frank psychosis appears.
Dopamine, NMDA and the Neurobiology of Prediction
Predictive coding also helps integrate neurotransmitter theories.
Dopamine may influence the precision of prediction errors. When dopamine signaling is dysregulated, irrelevant events may be given excessive importance. This can contribute to aberrant salience, paranoia and delusional meaning.
NMDA receptor hypofunction may impair top-down predictions and cortical integration. If higher cortical systems cannot provide stable predictions, lower-level sensory signals may become noisy, fragmented or excessively influential.
GABAergic dysfunction may further disturb cortical excitation-inhibition balance, affecting how prediction errors are generated and regulated.
Thus, predictive coding does not replace dopamine or glutamate theories. It gives them a larger framework.
Dopamine answers: “Why does this feel important?”
NMDA dysfunction answers: “Why are predictions unstable?”
Corollary discharge answers: “Why does this not feel self-generated?”
Self-disorder answers: “What does this feel like from the inside?”
Together, they offer a richer model of schizophrenia.
Why This Matters Clinically
Predictive coding is not just an abstract theory. It can improve clinical understanding.
First, it reduces stigma. Psychosis can be understood as a disturbance in inference rather than as irrationality or moral failure.
Second, it explains why patients are convinced by their experiences. Their brain is not merely producing false beliefs; it is generating abnormal salience and abnormal perception.
Third, it helps clinicians avoid premature confrontation. If a delusion is serving as an explanation for frightening prediction errors, directly attacking the belief may increase distress. A better approach is to gently explore the experience beneath the belief.
Fourth, it encourages early intervention. Subtle self-disorders, agency disturbances and unusual salience experiences may precede frank psychosis.
Fifth, it opens the door to personalized treatment. Future computational psychiatry may allow us to identify whether a patient’s symptoms are driven more by sensory instability, strong high-level priors, corollary discharge failure, aberrant salience or self-disorder.
A Simple Clinical Formulation
A clinically useful formulation may look like this:
A biologically vulnerable brain develops unstable predictive processing. Prior expectations become unreliable, while sensory prediction errors are given excessive importance. Ordinary events begin to feel unusually meaningful. Internally generated thoughts or sensations may not be properly recognized as self-generated. The person experiences confusion, perplexity, altered selfhood and heightened salience. Delusions and hallucinations emerge as attempts to explain these altered experiences.
This formulation is more compassionate than simply saying, “The patient has false beliefs.” It recognizes that psychotic symptoms are meaningful attempts to make sense of a changed experiential world.
Conclusion: Psychosis as a Disorder of Inference, Agency and Selfhood
Predictive coding offers one of the most promising modern frameworks for understanding psychosis. It does not reduce schizophrenia to dopamine, hallucinations or delusions. Instead, it explains how brain systems involved in prediction, precision, agency and belief formation may become disturbed.
In this view, psychosis is not merely a disorder of thought. It is a disorder of inference.
The brain misjudges what to trust: expectation, sensation, coincidence, memory, inner speech or social cues. As this imbalance grows, ordinary reality becomes unstable. The world feels charged with meaning. Thoughts may lose their sense of ownership. Voices may emerge from inner speech. Delusions may form as explanations for experiences that feel intensely real.
This model also brings together biological psychiatry and phenomenology. It helps us understand not only what the brain is doing, but also what the patient is living through.
For clinicians, the message is clear: when treating psychosis, we must go beyond symptom checklists. We must listen carefully to changes in selfhood, agency, salience and the patient’s lived experience of reality.
About the Author
Dr. Srinivas Rajkumar T, MD, DNB, MBA
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery, Chennai
For appointments: +91-8595155808
Website: srinivasaiims.com