Neurobiology of Psychosis in the Elderly
 Psychosis in the elderly is not one single biological entity. In younger adults, new-onset psychosis often raises the possibility of schizophrenia-spectrum illness. In older adults, especially after 60 years, psychosis is more often a final common pathway of several interacting vulnerabilities:
Psychosis in the elderly is not one single biological entity. In younger adults, new-onset psychosis often raises the possibility of schizophrenia-spectrum illness. In older adults, especially after 60 years, psychosis is more often a final common pathway of several interacting vulnerabilities:
ageing brain + neurodegeneration + vascular disease + sensory impairment + neurotransmitter imbalance + medical illness + medications + psychosocial stress.
A recent review notes that late-onset psychosis has many possible causes and requires careful diagnosis because older adults are more vulnerable to adverse effects of antipsychotics. Another review reports that primary psychiatric disorders account for less than half of late-life psychotic symptoms, while up to 60% may be due to systemic medical or neurological conditions, especially neurodegenerative disorders.
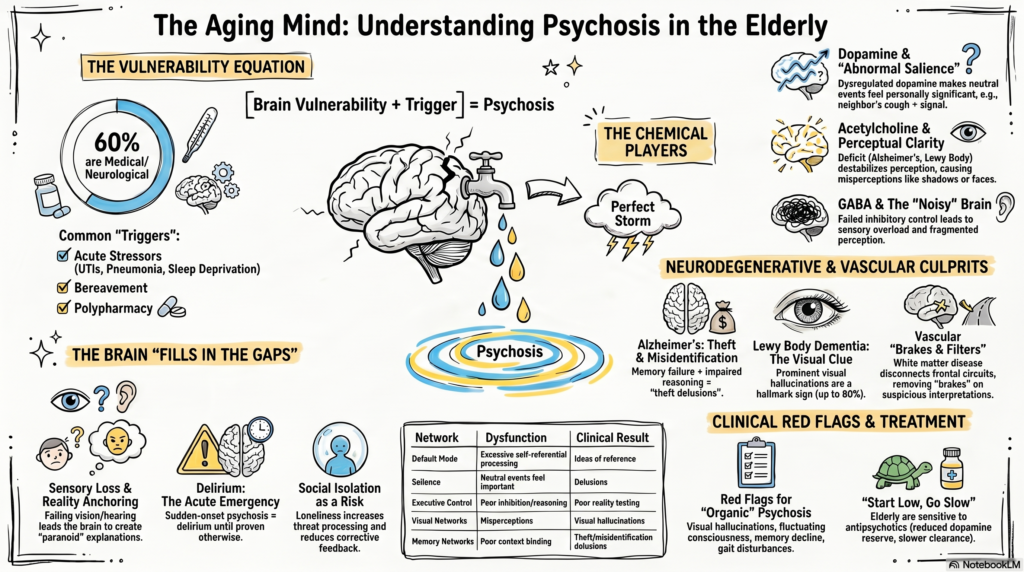
1. First principle: elderly psychosis is often “brain vulnerability + trigger”
In the elderly, psychosis commonly emerges when a vulnerable brain is pushed beyond its compensatory reserve.
Common vulnerabilities include:
| Vulnerability | Effect |
|---|---|
| Brain ageing | Reduced cognitive reserve |
| Dementia pathology | Misinterpretation, hallucinations, delusions |
| Vascular disease | Frontal-subcortical disconnection |
| Sensory loss | Reduced reality anchoring |
| Sleep disruption | Perceptual instability |
| Polypharmacy | Delirium, hallucinations |
| Social isolation | Paranoid meaning-making |
| Depression/anxiety | Mood-congruent psychotic ideas |
So the question is not only:
“Is this schizophrenia?”
It is also:
“What has changed in the brain, body, environment, medication list, sleep, vision, hearing, and cognition?”
2. Ageing brain and reduced cognitive reserve
With ageing, the brain has less reserve to compensate for biological stress.
There may be:
- cortical thinning
- reduced synaptic plasticity
- slower processing speed
- reduced inhibitory control
- impaired sleep architecture
- frontal-subcortical inefficiency
- accumulation of vascular and neurodegenerative pathology
This makes older adults more vulnerable to psychotic symptoms when exposed to stressors such as infection, insomnia, bereavement, medications, pain, sensory deprivation, or metabolic disturbance.
A younger brain may tolerate the same stressor without psychosis. An ageing brain may not.
3. Dopamine: abnormal salience, but with ageing sensitivity
Dopamine remains important in elderly psychosis, but the story is different from classic early-onset schizophrenia.
Dopamine helps assign salience:
“This is important.”
“Pay attention.”
“This has meaning.”
When dopamine signalling becomes dysregulated, neutral events may feel personally significant.
Clinical examples:
- “The neighbour’s cough is a signal.”
- “The television is giving me messages.”
- “People are watching me.”
- “The maid is stealing things.”
- “My family is plotting against me.”
In elderly patients, the dopamine system may be more sensitive to medications and brain disease. Even small dopaminergic shifts can produce psychosis.
This is why psychosis may occur with:
- Parkinson’s disease medications
- dopamine agonists
- levodopa
- stimulants
- some antidepressant activating states
- steroids
- delirium states
In elderly patients, dopamine dysregulation often interacts with cholinergic failure, vascular disconnection, and cognitive impairment.
4. Cholinergic deficit: especially important in dementia psychosis
Acetylcholine is crucial for:
- attention
- memory
- perceptual clarity
- REM sleep regulation
- visual processing
- reality monitoring
Cholinergic deficits are especially relevant in:
- Alzheimer’s disease
- dementia with Lewy bodies
- Parkinson’s disease dementia
- delirium
When acetylcholine is low, the brain’s perceptual system becomes less stable. The person may misperceive shadows, objects, faces, or sounds.
This is particularly important for visual hallucinations.
In dementia with Lewy bodies, psychosis is very common, often including presence hallucinations, passage hallucinations, and well-formed visual hallucinations; a recent neurology review describes psychosis as a prevalent and early neuropsychiatric symptom in Lewy body dementia, affecting up to 80% over the disease course.
Clinical clue:
Prominent visual hallucinations in an elderly person should immediately raise suspicion of Lewy body dementia, Parkinson’s disease dementia, delirium, medication effect, or visual impairment — not just schizophrenia.
5. Glutamate and NMDA dysfunction: impaired reality testing and cognition
Glutamate, especially NMDA receptor function, is important for:
- learning
- memory
- prediction
- cortical integration
- sensory processing
- synaptic plasticity
In psychosis, NMDA dysfunction may lead to poor integration of perception, memory, and meaning. The brain becomes less accurate in updating beliefs.
This can contribute to:
- delusions
- disorganised thinking
- cognitive impairment
- poor insight
- misinterpretation of stimuli
In the elderly, NMDA-glutamate dysfunction may be influenced by neurodegeneration, inflammation, metabolic illness, and vascular injury.
6. GABA and inhibitory failure
GABA is the main inhibitory neurotransmitter.
It helps the brain suppress irrelevant signals.
When GABAergic control is weak, the brain may become noisy.
The person may experience:
- sensory overload
- intrusive thoughts
- fragmented perception
- poor sleep
- agitation
- misinterpretation
In elderly psychosis, reduced inhibitory control may combine with sensory loss and cognitive decline.
This may produce a state where the brain fills in gaps with incorrect explanations.
7. Neurodegeneration: Alzheimer’s disease, Lewy body disease, Parkinson’s disease
This is one of the most important categories in elderly psychosis.
Alzheimer’s disease psychosis
Psychosis in Alzheimer’s disease may include:
- persecutory delusions
- theft delusions
- misidentification
- jealousy delusions
- hallucinations
- Capgras syndrome
The neurobiology often involves:
- medial temporal dysfunction
- frontal dysfunction
- impaired memory binding
- impaired reality monitoring
- cholinergic deficits
- amyloid/tau pathology
- network disconnection
A typical example:
The patient misplaces money due to memory impairment, then concludes: “Someone stole it.”
This is not simply paranoia. It is memory failure plus impaired contextual reasoning plus emotional salience.
Psychosis in Alzheimer’s disease is clinically important because it is associated with worse outcomes, caregiver burden, and faster decline in many studies. Reviews describe dementia-related psychosis as contributing to institutionalisation, cognitive decline, and caregiver burden.
Dementia with Lewy bodies
This is highly relevant when visual hallucinations are prominent.
Neurobiology:
- alpha-synuclein pathology
- cholinergic deficit
- dopaminergic dysfunction
- REM sleep dysregulation
- visual association cortex involvement
- attentional fluctuations
Clinical clues:
- recurrent visual hallucinations
- fluctuating cognition
- REM sleep behaviour disorder
- parkinsonism
- neuroleptic sensitivity
- presence hallucinations
- passage hallucinations
Important treatment implication:
Elderly patients with Lewy body dementia may be extremely sensitive to antipsychotics.
Parkinson’s disease psychosis
Usually related to a combination of:
- Parkinson’s disease pathology
- dopaminergic treatment
- cholinergic deficit
- sleep disturbance
- visual processing abnormalities
- cognitive decline
Clinical pattern:
- visual hallucinations
- illusions
- presence phenomena
- paranoid delusions
- medication-related worsening
The biological tension is difficult:
Dopamine replacement improves movement but can worsen psychosis.
Dopamine blockade reduces psychosis but can worsen parkinsonism.
8. Vascular brain disease and white matter disconnection
Vascular burden is a major contributor to late-life psychosis.
Small-vessel disease, lacunes, infarcts, and white matter hyperintensities can disrupt frontal-subcortical circuits.
This affects:
- judgment
- emotional regulation
- impulse control
- reality testing
- attention
- executive function
- belief updating
Vascular psychosis is often linked to cerebrovascular disease and late-onset psychotic symptoms in older adults. Older literature and reviews have also focused on white matter hyperintensities, vascular disease, and frontal/medial temporal dysfunction in late-life psychosis.
Clinical clues suggesting vascular contribution:
- late onset after 60
- executive dysfunction
- gait disturbance
- hypertension/diabetes history
- stepwise cognitive decline
- apathy or emotional lability
- MRI showing white matter disease
- poor frontal control of suspicious interpretations
A practical phrase:
White matter disease disconnects the brain’s “brakes and filters.”
9. Sensory impairment: the brain fills in missing data
Vision and hearing loss are often underestimated causes of psychosis-like experiences in older adults.
When sensory input becomes degraded, the brain may fill in missing information.
This can produce:
- visual illusions
- auditory misperceptions
- formed hallucinations
- paranoid interpretations
- social misunderstanding
Examples:
- Hearing loss: “They are whispering about me.”
- Cataract/poor vision: “I saw someone standing near the door.”
- Charles Bonnet syndrome: complex visual hallucinations with visual impairment and relatively preserved insight.
Sensory impairment does not “cause schizophrenia,” but it can reduce reality anchoring and increase paranoid explanations.
10. Delirium: acute psychosis in an inflamed/metabolically stressed brain
In elderly patients, acute psychosis must always raise the possibility of delirium.
Neurobiology of delirium includes:
- neuroinflammation
- cholinergic deficiency
- dopamine excess
- sleep-wake disruption
- metabolic disturbance
- blood-brain barrier vulnerability
- network disintegration
Common triggers:
- UTI
- pneumonia
- electrolyte imbalance
- hypoxia
- pain
- constipation
- urinary retention
- dehydration
- steroids
- anticholinergics
- benzodiazepines
- opioids
- sedative withdrawal
Clinical clues:
- acute onset
- fluctuating course
- worse at night
- inattention
- altered consciousness
- visual hallucinations
- disorientation
- new medical illness
In elderly psychiatry, the safest rule is:
New acute psychosis is delirium until proven otherwise.
11. Inflammation and immune activation
Ageing is associated with low-grade chronic inflammation, sometimes called “inflammaging.”
Inflammation can affect the brain by altering:
- dopamine metabolism
- glutamate signalling
- microglial activation
- blood-brain barrier function
- sleep
- mood
- cognition
This is relevant in:
- infections
- autoimmune illness
- post-operative states
- systemic inflammatory diseases
- neurodegenerative disorders
- frailty states
Inflammation may not directly “create delusions” in a simple way, but it destabilises attention, perception, sleep, and cognition — the background conditions in which psychosis can emerge.
12. Stress, loneliness, and threat processing
Elderly psychosis is not purely biological in a narrow sense. Social context shapes brain meaning-making.
Common psychosocial triggers:
- bereavement
- retirement
- isolation
- sensory deprivation
- dependency
- financial insecurity
- family conflict
- elder abuse
- migration or change of residence
These increase threat processing and reduce corrective feedback.
A lonely elderly person with hearing impairment and mild cognitive impairment may begin misinterpreting neutral events as hostile.
Clinical example:
“My son and daughter-in-law are planning to send me away.”
Sometimes this may be delusional. Sometimes it may be partially reality-based. Careful assessment is essential.
13. Late-onset schizophrenia-like psychosis
Some elderly patients develop psychosis without obvious dementia, delirium, or medical cause. This may be described as:
- late-onset schizophrenia: onset after 40
- very-late-onset schizophrenia-like psychosis: onset after 60
Clinical patterns often include:
- persecutory delusions
- partition delusions
- auditory hallucinations
- visual/tactile hallucinations may be more common than in early-onset schizophrenia
- fewer negative symptoms
- less formal thought disorder
- female predominance reported in many studies
- sensory impairment and social isolation as risk factors
Systematic reviews describe late-onset and very-late-onset schizophrenia-like psychosis as clinically distinct areas requiring attention to psychopathology, cognition, neurobiology, and psychosocial correlates.
Neurobiologically, this may involve:
- frontal-subcortical dysfunction
- temporal lobe vulnerability
- white matter changes
- sensory impairment
- dopamine sensitivity
- reduced cognitive reserve
14. Network-level explanation
At the network level, elderly psychosis may involve failure of coordination among:
| Network | Dysfunction | Clinical result |
|---|---|---|
| Default Mode Network | Excessive self-referential processing | Ideas of reference |
| Salience Network | Neutral events feel important | Delusions |
| Executive Control Network | Poor inhibition and reasoning | Poor reality testing |
| Visual networks | Misperceptions | Visual hallucinations |
| Limbic networks | Threat amplification | Paranoia |
| Memory networks | Poor context binding | Theft/misidentification delusions |
| Frontal-subcortical circuits | Poor updating and control | Fixed beliefs, disinhibition |
So elderly psychosis can be described as:
impaired perception + impaired memory + abnormal salience + reduced executive correction.
15. Why elderly patients are more sensitive to antipsychotics
The neurobiology of ageing also explains medication sensitivity.
Older adults have:
- reduced dopamine reserve
- higher extrapyramidal vulnerability
- more cholinergic deficits
- greater orthostatic risk
- slower hepatic/renal clearance
- more polypharmacy
- higher delirium risk
- greater cerebrovascular vulnerability
- dementia-related mortality warnings with antipsychotics
This is why the geriatric principle is:
Start low, go slow, but treat adequately when risk is significant.
Antipsychotics may be needed for dangerous distressing psychosis, but the threshold for medical workup, medication review, and non-pharmacological correction is much higher than in young adult psychosis.
16. Practical clinical formulation
For an elderly patient with psychosis, the biological formulation can be structured as:
A. Predisposing factors
- ageing brain
- family history
- sensory impairment
- cognitive impairment
- vascular burden
- neurodegenerative disease
- prior psychiatric illness
B. Precipitating factors
- infection
- insomnia
- bereavement
- pain
- medication change
- social isolation
- hospitalisation
- metabolic disturbance
C. Perpetuating factors
- untreated hearing/vision loss
- caregiver conflict
- ongoing sleep disruption
- delusional reinforcement
- cognitive decline
- polypharmacy
- loneliness
D. Protective factors
- family support
- routine
- sleep restoration
- sensory aids
- cognitive stimulation
- medical optimisation
- safe environment
17. Clinical red flags suggesting organic cause
In an elderly patient, psychosis is more likely organic when there is:
- first onset after 60
- visual hallucinations
- fluctuating consciousness
- disorientation
- memory decline
- neurological signs
- parkinsonism
- gait disturbance
- seizures
- headache
- recent medication change
- fever/infection
- sudden onset
- autonomic symptoms
- substance or sedative use
- anticholinergic burden
Summary
Psychosis in the elderly is usually a disorder of reduced brain reserve, where neurodegeneration, vascular disconnection, neurotransmitter imbalance, sensory loss, inflammation, and psychosocial stress converge to disturb perception, salience, memory, and reality testing.
In young psychosis, we often think:
dopamine + neurodevelopment + salience.
In elderly psychosis, we must think:
dopamine + cholinergic failure + dementia + vascular brain disease + sensory loss + delirium + medications + reduced cognitive reserve.
That is the core neurobiology of psychosis in the elderly.
Related posts:
- The Neurobiology of Exercise and Dance in Psychiatry: Unlocking Mental Health Benefits
- Neurobiology of Addiction – Impulsivity – Compulsivity
- Autism Spectrum Disorder (ASD) and Ketamine: Emerging Insights from Neurobiology to Potential Intervention
- Pimavanserin: A Breakthrough Treatment for Parkinson’s Disease Psychosis
- Parkinson’s Disease Caregiver Guide: Managing Depression and Psychosis
- Life After Psychosis: A Patient’s Journey Back to Reality