Esketamine vs rTMS in Treatment-Resistant Depression: Which Provides Faster Relief?
 Treatment-resistant depression (TRD) remains one of the greatest challenges in modern psychiatry. While conventional antidepressants help many patients, a substantial proportion continue to experience persistent symptoms despite adequate medication trials.
Treatment-resistant depression (TRD) remains one of the greatest challenges in modern psychiatry. While conventional antidepressants help many patients, a substantial proportion continue to experience persistent symptoms despite adequate medication trials.
For these patients, two major evidence-based interventions have emerged over the past decade:
- Repetitive Transcranial Magnetic Stimulation (rTMS)
- Intranasal Esketamine
Both are approved for treatment-resistant depression and have transformed the treatment landscape. However, an important clinical question remains:
Which treatment works faster?
When a patient is severely depressed, unable to function, or experiencing suicidal thoughts, speed of response becomes as important as efficacy itself.
A recent 2026 study published in the Journal of Affective Disorders compared real-world outcomes in patients receiving rTMS and intranasal esketamine and provides valuable insights into this question.
Why Speed of Response Matters
In everyday clinical practice, psychiatrists are not merely treating depression scores. They are treating:
- Human suffering
- Occupational dysfunction
- Relationship breakdown
- Loss of quality of life
- Suicidal thoughts
For many patients, waiting six to eight weeks for meaningful improvement is simply too long.
The ideal intervention should therefore provide:
- Rapid symptom reduction
- Improvement in functioning
- Reduction in suicidal ideation
- Sustained long-term benefit
This is where esketamine and rTMS have generated significant interest.
Understanding the Two Treatments
What is rTMS?
Repetitive Transcranial Magnetic Stimulation is a non-invasive brain stimulation technique that uses rapidly changing magnetic fields to stimulate specific brain regions involved in mood regulation.
Most protocols target the dorsolateral prefrontal cortex, a region consistently implicated in depression.
rTMS:
✓ Non-drug treatment
✓ No anaesthesia required
✓ Minimal systemic side effects
✓ No cognitive impairment
✓ Typically delivered over 4–6 weeks
The treatment gradually modifies dysfunctional neural networks through repeated stimulation and neuroplastic changes.
What is Esketamine?
Esketamine is the S-enantiomer of ketamine administered as a nasal spray under medical supervision.
Unlike conventional antidepressants that act primarily on serotonin and noradrenaline pathways, esketamine acts on the glutamatergic system through NMDA receptor antagonism.
This leads to:
- Rapid synaptic remodeling
- Increased neuroplasticity
- Enhanced neuronal connectivity
- Fast antidepressant effects
Treatment is usually administered twice weekly during the induction phase, followed by maintenance sessions.
The Study
Researchers from the University of California San Diego examined outcomes from:
- 279 patients receiving rTMS
- 93 patients receiving intranasal esketamine
All patients met criteria for treatment-resistant depression and were treated in a real-world interventional psychiatry service.
Unlike tightly controlled clinical trials, this study reflects what psychiatrists encounter in routine practice.
Esketamine Produced Faster Antidepressant Response
The most striking finding was the difference in speed.
Median Time to Response
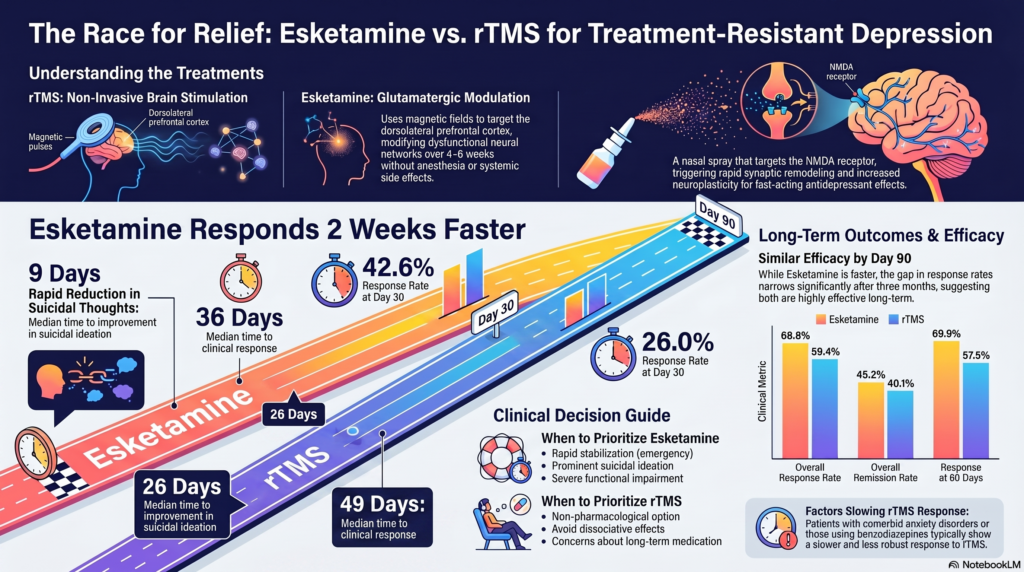
Esketamine: 36 days
rTMS: 49 days
In practical terms, patients receiving esketamine improved approximately two weeks earlier than patients receiving rTMS.
The advantage was particularly noticeable during the first month of treatment.
At 30 days:
- 42.6% of esketamine patients had responded
- 26.0% of rTMS patients had responded
At 60 days:
- 69.9% of esketamine patients had responded
- 57.5% of rTMS patients had responded
However, by approximately 90 days, the difference became much smaller.
This suggests that the major advantage of esketamine lies in speed rather than ultimate effectiveness.
Esketamine Reduced Suicidal Thoughts Faster
Perhaps the most clinically meaningful finding involved suicidal ideation.
Median Time to Improvement in Suicidal Thoughts
Esketamine: 9 days
rTMS: 26 days
This represents nearly a three-fold difference in speed.
Within just ten days:
- More than half of esketamine-treated patients demonstrated improvement in suicidal ideation
- Less than one quarter of rTMS patients had improved
For psychiatrists managing patients in acute distress, this finding has major implications.
When rapid reduction of suicidal thinking is a treatment priority, esketamine may offer a significant advantage.
Why Does Esketamine Work Faster?
The answer lies in neurobiology.
Traditional antidepressants primarily modify monoamine neurotransmitters such as serotonin and noradrenaline.
These downstream neuroadaptive changes often take several weeks.
Esketamine acts differently.
It directly influences glutamatergic neurotransmission and rapidly activates pathways involved in:
- Synaptic plasticity
- Neurogenesis
- Brain-derived neurotrophic factor (BDNF) signaling
- Cortical connectivity
This allows therapeutic effects to emerge far more quickly.
Many patients report meaningful improvement within days rather than weeks.
Does Faster Mean Better?
Not necessarily.
One of the most important messages from the study is that both treatments ultimately produced similar overall outcomes.
Overall Response Rates
Esketamine: 68.8%
rTMS: 59.4%
Remission Rates
Esketamine: 45.2%
rTMS: 40.1%
Although esketamine appeared numerically superior, the primary distinction was speed of improvement rather than dramatically greater efficacy.
By three months, both treatments achieved substantial clinical benefit.
Predictors of rTMS Response
The study also identified factors associated with slower rTMS improvement.
Anxiety Disorders
Patients with significant anxiety symptoms improved more slowly.
This observation is consistent with previous literature suggesting that anxiety may reduce rTMS effectiveness.
Benzodiazepine Use
Patients taking benzodiazepines showed slower and less robust responses to rTMS.
This is clinically important because benzodiazepines may interfere with the neuroplastic mechanisms through which rTMS exerts its therapeutic effects.
Whenever possible, psychiatrists may consider minimizing benzodiazepine burden before initiating rTMS.
Choosing the Right Treatment
The question is no longer:
“Which treatment is better?”
The more useful question is:
“Which treatment is better for this particular patient at this particular moment?”
Esketamine May Be Preferred When:
- Rapid relief is needed
- Suicidal ideation is prominent
- Functional impairment is severe
- Previous rTMS has failed
- The patient can comply with supervised administration
rTMS May Be Preferred When:
- A non-pharmacological treatment is desired
- Dissociative effects are undesirable
- Long-term medication exposure is a concern
- The patient prefers neuromodulation
- Esketamine is unavailable or unaffordable
The Future: Not Either-Or, But Personalized Psychiatry
The future of interventional psychiatry is unlikely to involve choosing a single “best” treatment.
Instead, clinicians will increasingly tailor interventions based on:
- Clinical presentation
- Urgency of symptoms
- Suicidal risk
- Comorbid anxiety
- Previous treatment history
- Biomarkers and neurophysiology
For some patients, esketamine may provide rapid stabilization followed by rTMS for longer-term maintenance.
For others, rTMS alone may be sufficient.
The goal is individualized care rather than a one-size-fits-all approach.
Key Take-Home Messages
✓ Esketamine produces faster antidepressant effects than conventional rTMS.
✓ Median response occurs approximately two weeks earlier with esketamine.
✓ Improvement in suicidal ideation occurs substantially faster with esketamine.
✓ By approximately three months, overall outcomes between treatments become similar.
✓ Anxiety disorders and benzodiazepine use may predict slower rTMS response.
✓ Treatment selection should be individualized based on clinical urgency, patient preference, safety considerations, and long-term goals.
As interventional psychiatry continues to evolve, both esketamine and rTMS represent powerful tools in the management of treatment-resistant depression. The challenge for clinicians is no longer whether these treatments work, but identifying which patient is most likely to benefit from which intervention and when.
Dr. Srinivas Rajkumar T
MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery, Chennai
Opp. Phoenix Mall
Email: srinivasaiims@gmail.com
Phone: +91-8595155808
Based on: Benster LL et al. Comparing transcranial magnetic stimulation and esketamine treatment response trajectories in resistant depression. Journal of Affective Disorders, 2026.