EUPD, Borderline Personality Disorder, Mood Changes, PCOS and Periods: Why Hormonal Patterns Should Not Be Missed
 Emotionally Unstable Personality Disorder, also called Borderline Personality Disorder, is often described through emotional intensity, relationship sensitivity, fear of abandonment, impulsivity, anger, self-harm risk and rapid mood shifts. But in many women, one important layer is missed:
Emotionally Unstable Personality Disorder, also called Borderline Personality Disorder, is often described through emotional intensity, relationship sensitivity, fear of abandonment, impulsivity, anger, self-harm risk and rapid mood shifts. But in many women, one important layer is missed:
symptoms may worsen predictably around the menstrual cycle.
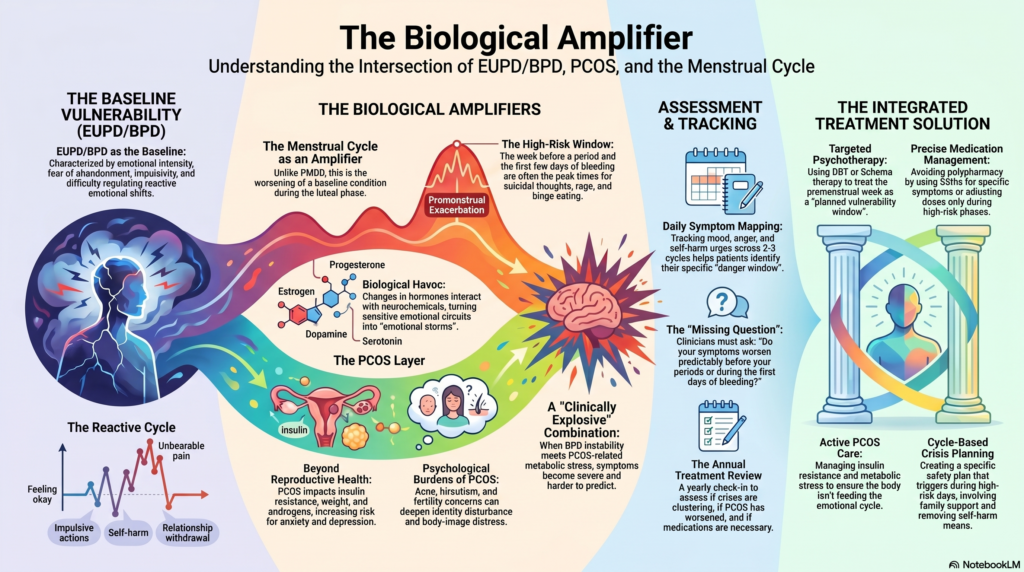
This does not mean that EUPD/BPD is “just hormones.” It is not. BPD is a complex disorder of emotional regulation, attachment sensitivity, identity disturbance, impulse control and interpersonal functioning. But hormonal shifts can act like a biological amplifier. In some patients, the week before periods and the first few days of bleeding can become a high-risk window for emotional storms, rejection sensitivity, anger, crying spells, impulsivity, suicidal thoughts, self-harm urges, binge eating, sleep disturbance and relationship conflict.
When this pattern is missed, the person may be labelled as “dramatic,” “manipulative,” “non-compliant,” or “treatment resistant.” In reality, part of the problem may be that nobody has mapped the interaction between EUPD/BPD, menstrual-cycle-related mood change, PMDD-like symptoms and PCOS.
EUPD/BPD: the baseline vulnerability
EUPD/BPD is characterised by difficulty regulating emotions, intense and unstable relationships, impulsivity, fear of abandonment, anger, identity disturbance and sometimes self-harm. NICE describes borderline personality disorder as a condition involving distress, anxiety, worthlessness, anger and difficulties maintaining stable relationships.
The emotional shifts in BPD are usually reactive. A message not replied to, a perceived slight, criticism, loneliness, uncertainty or fear of abandonment may trigger intense emotional pain.
The person may move rapidly from:
“I am okay”
to
“Nobody cares about me”
to
“I cannot tolerate this feeling”
to
“I need to do something immediately to reduce this pain.”
That “something” may be repeated calls, angry messages, self-harm, substance use, binge eating, impulsive spending, quitting a relationship, or suddenly withdrawing.
This baseline vulnerability exists throughout the month. But in many women, it becomes more intense around the menstrual cycle.
The missing question: “Does this worsen before periods?”
In routine psychiatric practice, clinicians often ask about mood, sleep, appetite, anger, self-harm, trauma, substance use and relationships. But they may forget to ask a simple question:
“Do these symptoms worsen before your periods or during the first few days of bleeding?”
This is a major missed opportunity.
A study on perimenstrual exacerbation in women with BPD found that women with BPD may be at increased risk of worsening emotional symptoms around the menstrual phase. The authors specifically highlighted the need for more longitudinal work with detailed hormonal measurement.
This is clinically important because many women do not volunteer this information. They may think it is “normal PMS.” Families may dismiss it as “monthly moodiness.” Doctors may focus only on the personality diagnosis and miss the cyclical pattern.
But when symptoms become severe enough to cause self-harm urges, relationship breakdown, rage episodes, suicidal thoughts, absenteeism, binge eating or emergency consultations, it is no longer trivial.
PMS, PMDD and premenstrual exacerbation are not the same
There are three overlapping but distinct ideas.
PMS refers to physical and emotional symptoms before periods. Many women experience some degree of PMS.
PMDD, or Premenstrual Dysphoric Disorder, is more severe. It involves marked mood symptoms such as irritability, depression, anxiety, mood swings and functional impairment in the luteal phase, usually improving after menstruation begins. ACOG’s 2023 clinical practice guideline discusses evidence-based treatment options for premenstrual disorders, including PMS and PMDD.
Premenstrual exacerbation means that an existing psychiatric condition worsens premenstrually. In this situation, the person already has BPD, depression, bipolar disorder, anxiety, OCD or another condition, but the symptoms flare up before periods.
This distinction matters.
A woman with pure PMDD may be relatively well for much of the month and become severely symptomatic only in the premenstrual phase. A woman with EUPD/BPD may have emotional sensitivity throughout the month, but the premenstrual window may push her from “struggling but managing” to “unsafe, impulsive or overwhelmed.”
Why periods can “wreak havoc” in EUPD/BPD
The menstrual cycle involves changing levels of estrogen, progesterone and their neuroactive metabolites. These interact with serotonin, GABA, dopamine, stress-response systems and emotional regulation circuits.
In someone without major emotional regulation difficulty, these changes may produce mild irritability, fatigue or sadness. In someone with EUPD/BPD, the same biological shifts may interact with already sensitive emotional circuits.
The result may be:
more rejection sensitivity,
more anger,
more crying spells,
more impulsive communication,
more self-harm urges,
more binge eating,
more sleep disturbance,
more body-image distress,
more interpersonal conflict,
more suicidal thoughts.
This is why a patient may say:
“I was doing well, then suddenly I became a different person before my periods.”
“I fight with everyone only during that week.”
“My self-harm urges come before periods.”
“I feel abandoned and unloved before my cycle.”
“I know I overreact, but in that moment it feels unbearable.”
The psychiatrist must not dismiss this as “just PMS.” In high-risk patients, the menstrual cycle can be a predictable biological vulnerability window.
Where PCOS enters the picture
Polycystic Ovary Syndrome, or PCOS, is not only a reproductive or cosmetic condition. It can affect weight, insulin resistance, acne, hair growth, body image, fertility, sleep, metabolic risk and mood.
The 2023 International Evidence-based Guideline for PCOS states that depressive and anxiety symptoms are significantly increased in women with PCOS and should be screened for, with psychological assessment and therapy considered as part of care.
PCOS may worsen emotional health through multiple pathways:
irregular periods,
androgen-related symptoms such as acne or hirsutism,
weight gain and insulin resistance,
body-image distress,
fertility worries,
sleep disturbance,
inflammation and metabolic stress,
repeated medical invalidation,
and chronic shame.
For a woman with EUPD/BPD, PCOS can become an additional burden on identity, body image, self-esteem and relationships. If she already struggles with abandonment sensitivity and emotional regulation, PCOS-related distress can deepen the emotional load.
Why PCOS plus EUPD/BPD can be clinically explosive
In EUPD/BPD, the emotional system is highly reactive. In PCOS, the body may be sending repeated signals of hormonal, metabolic and reproductive irregularity. When both coexist, the patient may experience a layered vulnerability.
There may be:
baseline emotional dysregulation,
premenstrual worsening,
irregular cycles that make mood changes harder to predict,
body-image distress,
acne or hair growth affecting self-esteem,
weight-related shame,
relationship insecurity,
fear about fertility,
binge eating or restrictive eating,
sleep disruption,
and insulin-resistance-related fatigue.
This can look like “borderline instability,” but that label alone is incomplete. The better formulation is:
A person with emotional regulation vulnerability whose symptoms are amplified by cyclical hormonal changes and PCOS-related psychological and metabolic stress.
That formulation is more humane. It also opens the door to better treatment.
Why clinicians miss this pattern
This pattern is often missed for several reasons.
First, psychiatric consultations may focus on crisis events: self-harm, anger outbursts, relationship fights, suicidal ideation, substance use or impulsivity. The timing of the crisis is not mapped.
Second, menstrual history is often taken only in gynaecology, not psychiatry.
Third, PCOS is often reduced to irregular periods, acne, weight and fertility. Its psychological effects are under-discussed.
Fourth, BPD is a stigmatised diagnosis. Once the label is applied, every symptom may be attributed to “personality,” even when there are treatable biological contributors.
Fifth, patients themselves may not see the pattern unless they track it. When someone is emotionally overwhelmed, it is difficult to remember whether the same thing happened around the same phase last month.
The annual review: why yearly treatment planning matters
For women with EUPD/BPD, PCOS and menstrual-cycle-related mood changes, treatment should not be a one-time prescription. It needs periodic review, at least yearly, and more frequently when symptoms are severe.
A yearly review should ask:
Have mood symptoms changed over the past year?
Are crises clustering before periods?
Are periods regular or irregular?
Has PCOS worsened?
Is weight, acne, hirsutism or body image affecting mood?
Are there binge-eating patterns?
Are there self-harm urges before periods?
Is contraception affecting mood?
Is the patient on unnecessary long-term sedatives or mood stabilisers?
Is psychotherapy progressing?
Are antidepressants helping?
Is there bipolarity, ADHD, trauma, substance use or eating disorder comorbidity?
Is the gynaecological plan aligned with the psychiatric plan?
NICE recommends that when treating BPD, clinicians should monitor a broad range of outcomes including personal functioning, drug and alcohol use, self-harm, depression and BPD symptoms. NICE also advises reviewing unnecessary drug treatment in people with BPD who do not have a diagnosed comorbid mental or physical illness.
This is particularly relevant here. Many patients with EUPD/BPD are placed on multiple medications over time, especially after crises. A yearly review helps separate what is truly helping from what is simply accumulating.
What should be assessed in such patients?
A good assessment should include both psychiatric and hormonal/metabolic dimensions.
Psychiatric assessment
The psychiatrist should assess:
emotional dysregulation,
self-harm and suicide risk,
impulsivity,
anger,
relationship instability,
identity disturbance,
trauma history,
depression,
anxiety,
bipolar spectrum symptoms,
ADHD symptoms,
substance use,
eating patterns,
sleep,
and functioning.
Menstrual-cycle assessment
The psychiatrist should ask:
Are symptoms worse before periods?
How many days before bleeding do they start?
Do symptoms improve after bleeding begins?
Are there high-risk days for self-harm or suicidal thoughts?
Are periods regular?
Is there severe pain or heavy bleeding?
Is there premenstrual insomnia, rage, binge eating or panic?
Has contraception changed mood?
PCOS-related assessment
The assessment should include:
cycle regularity,
weight changes,
acne,
hirsutism,
hair fall,
insulin resistance,
diabetes risk,
sleep apnoea symptoms,
body image,
fertility concerns,
exercise pattern,
dietary distress,
and gynaecology/endocrinology care.
Tracking
The simplest and most powerful tool is daily tracking for two to three cycles.
Track:
mood, anger, anxiety, sleep, self-harm urges, impulsivity, binge eating, conflicts, bleeding days, pain, fatigue and medication changes.
This can transform treatment. Instead of saying “I am always unstable,” the patient may discover:
“My danger window is day -7 to day +2.”
That changes everything.
Treatment: not either personality or hormones, but both
Treatment should be integrated. The mistake is to choose one explanation and ignore the other.
It is not helpful to say:
“This is only BPD.”
or
“This is only hormones.”
A better approach is:
Treat the emotional regulation disorder, identify menstrual-cycle amplification, manage PCOS, and build a crisis plan around high-risk days.
1. Psychotherapy remains central
For EUPD/BPD, psychotherapy is foundational. Evidence-based approaches include DBT, mentalisation-based therapy, schema therapy, transference-focused psychotherapy and structured clinical management.
The goals include:
emotion regulation,
distress tolerance,
interpersonal effectiveness,
identity strengthening,
reducing self-harm,
understanding triggers,
improving reflective capacity,
and building a life worth living.
When there is menstrual worsening, therapy can become more targeted. The patient can learn to treat the premenstrual week as a planned vulnerability window rather than a surprise attack.
For example:
avoid major relationship decisions during high-risk days,
delay impulsive messages,
increase sleep protection,
reduce alcohol,
schedule therapy check-ins,
use DBT crisis skills,
ask family for low-conflict support,
and prepare a self-harm safety plan.
2. Medication should be precise, not excessive
There is no single “BPD tablet.” Medication may help specific symptoms or comorbidities, but polypharmacy can worsen fatigue, weight, cognition and emotional blunting.
Medication decisions may involve:
SSRIs for comorbid depression, anxiety or PMDD-like symptoms,
short-term medication for severe insomnia or agitation with caution,
treatment of bipolar disorder if clearly present,
ADHD treatment if comorbid ADHD is diagnosed,
and careful avoidance of unnecessary long-term sedative dependence.
For PMDD and premenstrual disorders, ACOG’s 2023 guideline includes evidence-based treatment options such as SSRIs, hormonal management, psychological interventions and lifestyle approaches.
In a patient with EUPD/BPD, the psychiatrist must individualise treatment. Some may need continuous SSRI treatment. Some may benefit from premenstrual dose adjustments. Some may not tolerate hormonal contraception well. Some may need gynaecology collaboration. The plan should be based on symptom tracking, diagnosis and risk.
3. PCOS must be actively treated
If PCOS is present, it should not be ignored by the psychiatrist.
PCOS management may involve gynaecology/endocrinology input, lifestyle changes, weight and metabolic care, insulin resistance management, cycle regulation, acne/hirsutism treatment, fertility counselling when needed, and screening for depression, anxiety, eating disorders and body-image distress.
The 2023 international PCOS guideline emphasises best-practice assessment and management with multidisciplinary input and attention to psychological features.
In psychiatry, the point is not to manage PCOS alone, but to ensure it is not treated as irrelevant. For some patients, untreated PCOS keeps feeding the emotional cycle.
4. Crisis planning around the menstrual window
For patients with self-harm risk, suicidal thoughts or severe rage episodes before periods, the high-risk window should be built into the care plan.
A crisis plan may include:
warning signs,
cycle-based risk days,
sleep protection,
avoiding alcohol or drugs,
limiting late-night conflict,
removing access to self-harm means,
emergency contact plan,
therapy skills list,
family instructions,
and follow-up timing.
This is not overmedicalising periods. It is harm reduction.
If a patient has predictable worsening every month, the treatment system should become predictable too.
5. Family psychoeducation is essential
Families often experience the premenstrual worsening as chaos. They may respond with criticism, anger or helplessness.
The family needs to understand:
the patient is responsible for learning skills,
but the symptoms are not simply “drama,”
hormonal shifts can amplify emotional pain,
PCOS can worsen body image and mood,
invalidating comments can escalate crises,
and predictable high-risk days need predictable support.
Family members can be taught to reduce emotional escalation, avoid provocative arguments during vulnerable days, support sleep, encourage treatment adherence, and respond calmly to self-harm threats without either panic or dismissal.
Red flags that need urgent psychiatric attention
Seek urgent help if there is:
suicidal ideation,
self-harm,
violent impulses,
severe insomnia,
psychotic symptoms,
substance intoxication,
repeated emergency crises before periods,
severe bingeing or purging,
or inability to function during the premenstrual phase.
Severe premenstrual worsening in someone with EUPD/BPD should not be dismissed as routine PMS.
A better clinical formulation
Instead of saying:
“She is borderline and hormonal.”
A better formulation is:
“She has EUPD/BPD with emotional regulation vulnerability, and her symptoms show premenstrual exacerbation. PCOS may be contributing through irregular cycles, metabolic stress, body-image distress and mood vulnerability. Treatment should combine psychotherapy, cycle tracking, PCOS care, careful medication review and a menstrual-window crisis plan.”
This formulation is more accurate, more respectful and more treatable.
Patient-friendly summary
Women with EUPD/BPD may experience significant mood worsening before periods. PCOS can add further stress through irregular cycles, acne, weight changes, insulin resistance, body-image concerns and fertility worries. If this pattern is missed, the person may be wrongly seen as simply “unstable” or “difficult.”
The key is to track symptoms across the cycle, treat EUPD/BPD with structured psychotherapy, manage PCOS properly, review medication yearly, and create a plan for high-risk premenstrual days.
Periods do not cause BPD.
PCOS does not cause all mood problems.
But hormones and PCOS can amplify emotional dysregulation.
Missing this means missing a major treatment opportunity.
Conclusion
EUPD/BPD is a serious emotional regulation disorder. PCOS is a serious endocrine-metabolic condition. Premenstrual mood worsening is a serious clinical pattern. When all three overlap, patients can suffer for years without a proper formulation.
The future of women’s mental health care must be integrated. Psychiatry should not ignore the menstrual cycle. Gynaecology should not ignore mood and self-harm. PCOS care should not stop with ultrasound and hormones. BPD care should not stop with crisis labels and medications.
The right approach is compassionate, structured and biologically informed:
track the cycle, understand the personality pattern, treat PCOS, review yearly, reduce risk and build emotional regulation skills.
That is how we move from blame to treatment.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
Related posts:
- Emotionally Unstable Personality Disorder (EUPD): Understanding What Lies Beneath the Pain
- More Than Hormones – Understanding Perimenopausal Mood Changes
- The Bottomless Pit: Why You’ll Never Feel ‘Enough’ in Borderline Personality Disorder
- The Borderline Mother and the Making of the Borderline Self: Insights from James F. Masterson
- 5 Effective Techniques to Manage Emotions in Borderline Personality Disorder (BPD)
- Communication Paradoxes in Borderline Personality Disorder: Expanding on Ruffalo’s Framework