Thought–Action Fusion in OCD: When Thoughts Feel Dangerous, Immoral, or Real
 Among the many cognitive distortions seen in Obsessive-Compulsive Disorder (OCD), Thought–Action Fusion (TAF) stands out as one of the most distressing—particularly for patients who experience aggressive, sexual, or blasphemous thoughts directed toward loved ones or sacred figures.
Among the many cognitive distortions seen in Obsessive-Compulsive Disorder (OCD), Thought–Action Fusion (TAF) stands out as one of the most distressing—particularly for patients who experience aggressive, sexual, or blasphemous thoughts directed toward loved ones or sacred figures.
These are often the patients who say, with visible anguish:
- “What if I harm my child?”
- “Why did I think something bad about God?”
- “Does this mean I am capable of doing it?”
- “What kind of person thinks like this?”
What they are not describing is intent.
They are describing a collapse between thought and meaning.
What is Thought–Action Fusion?
TAF refers to a cognitive distortion where an individual believes that:
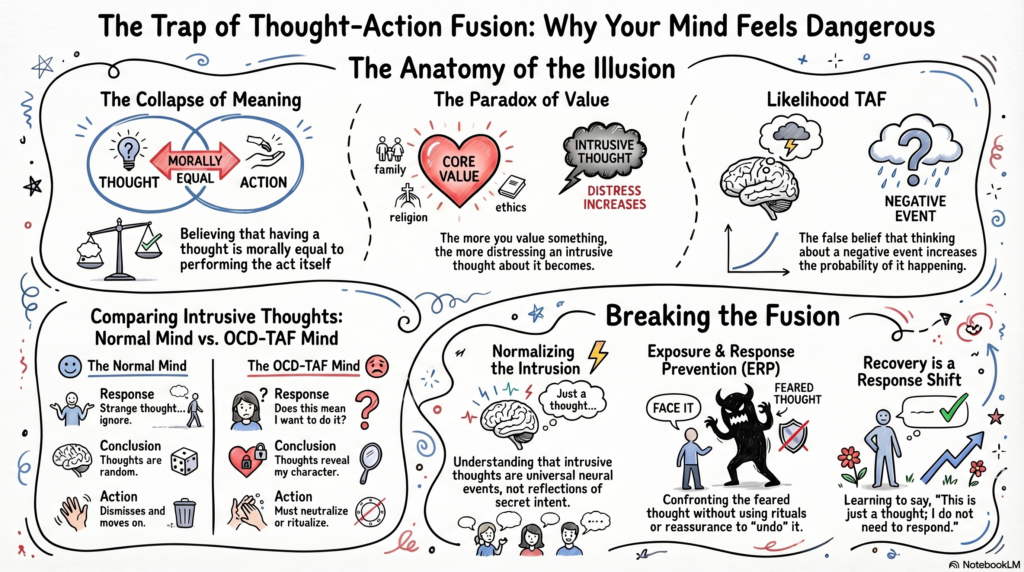
1. Thinking about an act is morally equivalent to performing it
(Moral TAF)
“If I think something blasphemous, I have already sinned.”
2. Thinking about an event increases the likelihood of it occurring
(Likelihood TAF)
“If I imagine harming my loved one, it may actually happen.”
These beliefs are not merely intellectual—they are felt with conviction, often accompanied by intense guilt, fear, and a need to neutralize the thought.
Why This Hits Hardest in “Forbidden” Thoughts
TAF is particularly severe when the content of the thought violates:
- Core moral values (violence, sexuality, betrayal)
- Religious beliefs (blasphemy, sacrilege)
- Attachment bonds (harm toward loved ones)
The paradox is striking:
➡️ The more a person values something,
➡️ the more distressing the intrusive thought becomes,
➡️ the stronger the TAF response.
A devoted parent may have a fleeting intrusive image of harming their child.
A religious individual may experience a sudden blasphemous phrase.
A caring partner may imagine betrayal.
These are ego-dystonic intrusions—they go against the person’s identity.
But under TAF, the mind says:
- “You thought it → it must mean something”
- “You thought it → you are capable of it”
- “You thought it → you are responsible for it”
The Normal Mind vs The OCD Mind
Intrusive thoughts are universal.
A non-OCD response:
- “Strange thought… ignore.”
An OCD-TAF response:
- “Why did I think this?”
- “Does this mean I want it?”
- “What if I act on it?”
- “I must neutralize this.”
The difference is not the thought.
It is the interpretation.
Clinical Phenotypes of TAF
1. Aggressive TAF
- Thoughts of harming children, spouses, or strangers
- Avoidance of knives, isolation, or being alone with loved ones
- Reassurance seeking: “I would never do this, right?”
2. Blasphemous / Scrupulosity TAF
- Intrusive thoughts insulting God or sacred figures
- Excessive praying, confession, ritual purification
- Fear of divine punishment
3. Sexual / Moral TAF
- Intrusive inappropriate sexual thoughts (often misinterpreted as desire)
- Intense shame and identity questioning
The Emotional Signature
Patients with TAF often present with:
- Guilt (“I am a bad person”)
- Fear (“What if I lose control?”)
- Shame (“I cannot tell anyone this”)
- Hypervigilance toward thoughts
- Compulsive neutralization (praying, repeating, avoiding, checking)
Importantly:
➡️ These patients are often least likely to act on these thoughts
➡️ Because the thoughts are profoundly ego-dystonic
The Cognitive Error
TAF rests on a fundamental misunderstanding of mental events:
1. Thoughts are treated as actions
2. Thoughts are treated as intentions
3. Thoughts are treated as predictors of behavior
In reality:
- Thoughts are spontaneous neural events
- They do not reflect intent
- They do not cause outcomes
- They do not define character
The Role of Control—and Its Failure
Many patients respond to these thoughts by trying to:
- Suppress them
- Replace them with “good thoughts”
- Neutralize them with rituals
This leads to the classic paradox:
The more you try not to think something, the more it appears.
This is not a failure of willpower.
It is a feature of cognitive control systems.
How Therapy Addresses Thought–Action Fusion
1. Psychoeducation: Normalizing Intrusions
Patients are often relieved to learn:
- Intrusive aggressive/blasphemous thoughts are common
- Having a thought ≠ wanting it
- The content reflects what matters most to you, not your intent
2. Cognitive Restructuring
Key therapeutic shifts:
- “Does thinking increase probability?”
- “Is a thought morally equivalent to action?”
- “What evidence supports this belief?”
The goal is not blind reassurance—but recalibrating meaning.
3. Exposure and Response Prevention (ERP)
The gold standard.
Exposure:
- Deliberately confronting the feared thought
- Writing scripts (“I may harm someone”)
- Imaginal exposure for blasphemous content
Response Prevention:
- No neutralization
- No reassurance
- No mental undoing
Over time:
➡️ Anxiety reduces
➡️ Belief weakens
➡️ Thought loses power
4. Acceptance-Based Approaches
Instead of control:
- Allow thoughts to exist
- Observe without engagement
- Return to meaningful action
Key shift:
“I can have this thought—and not respond to it.”
5. Decoupling Thought from Identity
A crucial therapeutic move:
- Thoughts do not define character
- Intrusions are not confessions
- The mind generates content—it does not endorse it
A Deeper Clinical Insight
Patients with severe TAF are often:
- Highly conscientious
- Morally sensitive
- Deeply attached to loved ones
- Spiritually invested
Their suffering arises not from lack of values—but from values amplified beyond proportion.
In that sense, OCD is not a disorder of immorality—it is a disorder of misinterpreted morality.
What Recovery Looks Like
Not the disappearance of thoughts—but a transformation in response:
- “This is just a thought.”
- “It does not mean anything about me.”
- “I do not need to respond to this.”
- “I can tolerate the uncertainty.”
The thought may still come.
But it no longer commands action.
Final Reflection
Thought–Action Fusion traps individuals in a painful illusion:
That the mind is dangerous,
that thoughts are powerful,
that morality lies in mental purity.
Therapy gently dismantles this illusion—
not by suppressing thoughts,
but by restoring freedom in how one relates to them.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
Special interest in OCD, intrusive thoughts, and cognitive-behavioral interventions, integrating ERP, neurocognitive tools, and AI-assisted formulations for precise, patient-centered care.
📞 +91-8595155808
✉ srinivasaiims@gmail.com