Why Grounding Skills Often Work Better Than Mindfulness in the Beginning: Getting Started with DBT
 Many patients who come to the OPD with emotional instability, intense anger, self-harm urges, anxiety spirals or relationship-triggered mood shifts are quickly advised to “do mindfulness.” The advice is well-meaning. Mindfulness is a core part of Dialectical Behaviour Therapy, and DBT is an evidence-based treatment for emotional dysregulation, borderline personality disorder/EUPD, self-harm and related difficulties. Yale Medicine describes DBT as a treatment that helps people change patterns of behaviour, emotion, thought and interpersonal interaction associated with emotion regulation problems.
Many patients who come to the OPD with emotional instability, intense anger, self-harm urges, anxiety spirals or relationship-triggered mood shifts are quickly advised to “do mindfulness.” The advice is well-meaning. Mindfulness is a core part of Dialectical Behaviour Therapy, and DBT is an evidence-based treatment for emotional dysregulation, borderline personality disorder/EUPD, self-harm and related difficulties. Yale Medicine describes DBT as a treatment that helps people change patterns of behaviour, emotion, thought and interpersonal interaction associated with emotion regulation problems.
But in real clinical practice, many patients struggle with mindfulness in the beginning.
They say:
“I cannot sit with my thoughts.”
“My mind becomes louder when I close my eyes.”
“I get more restless when I try to meditate.”
“I know I should observe my emotions, but I get swallowed by them.”
“When I am angry or suicidal, mindfulness feels impossible.”
This is not failure. It is often a sign that the patient needs simpler, more mechanical, body-based skills first.
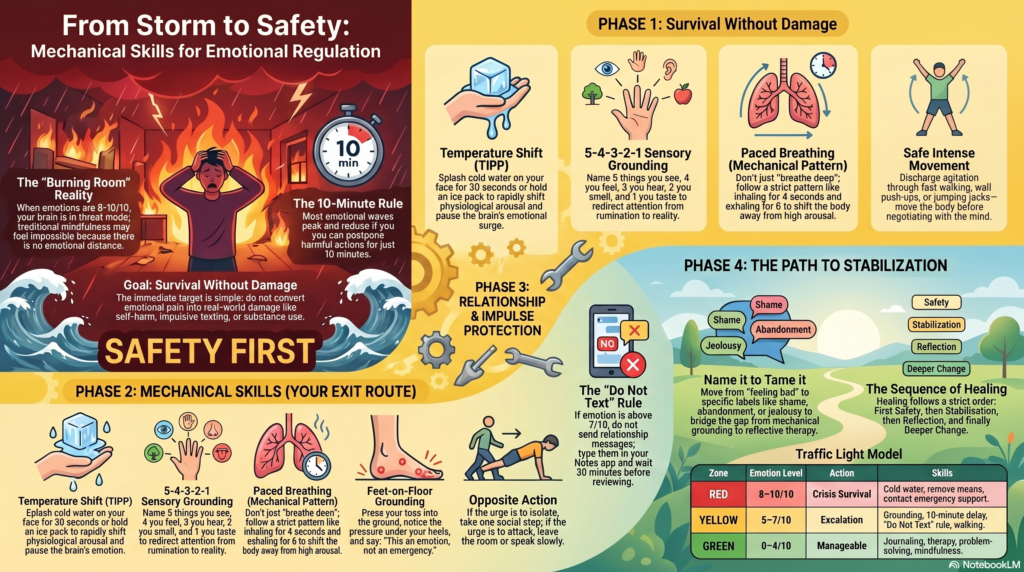
For many patients, especially those with EUPD/BPD traits, trauma histories, panic, self-harm urges or severe emotional reactivity, the first goal is not deep mindfulness. The first goal is survival without damage.
In the early phase of treatment, the question is not:
“Can I become calm and wise immediately?”
The first question is:
“Can I get through the next 10 minutes without harming myself, breaking a relationship, sending a destructive message, drinking, overdosing or making the situation worse?”
That is where grounding and DBT-style crisis-survival skills become extremely useful.
Why mindfulness may feel difficult initially
Mindfulness asks the person to observe thoughts, emotions and body sensations without immediately reacting. This is powerful, but it requires a certain degree of emotional distance.
In an emotional storm, that distance may not exist.
When the nervous system is highly activated, the person is not calmly “watching” anger or sadness. They are inside it. The brain is in threat mode. The body may feel unsafe. The person may be flooded by shame, rage, abandonment fear, panic or self-harm urges.
At that moment, telling the person to “just be mindful” may feel like asking someone in a burning room to appreciate the architecture.
They need an exit route first.
This is why early treatment often needs mechanical skills — things the patient can do with the body, senses, environment and behaviour, even when the mind is not cooperating.
What are mechanical skills?
Mechanical skills are simple, repeatable, physical or sensory actions that do not require deep insight in the moment.
They include:
cold water,
holding ice,
counting objects,
naming colours,
feet-on-floor grounding,
paced breathing,
walking,
muscle relaxation,
safe distraction,
urge delay,
moving away from triggers,
calling a support person,
writing instead of texting,
and creating a crisis card.
These skills are not “lesser” than mindfulness. They are often the entry point into emotional regulation.
DBT includes distress tolerance skills precisely for such situations. Reviews of DBT note that distress tolerance skills include crisis survival strategies that teach patients ways to get through intense distress without making things worse.
The first principle: do not make the crisis worse
In emotional dysregulation, the immediate urge is often to reduce pain quickly.
The person may feel like:
sending 40 messages,
calling repeatedly,
cutting,
banging the head,
drinking,
using substances,
breaking objects,
driving rashly,
threatening suicide,
quitting a job,
ending a relationship,
or posting something impulsively online.
These behaviours may briefly reduce emotional pressure, but they usually create new problems: shame, injury, conflict, hospitalisation, police issues, damaged relationships or deeper hopelessness.
So the first treatment target is simple:
Do not convert emotional pain into real-world damage.
Distress tolerance skills are meant for exactly this. A Kaiser Permanente DBT skills handout describes crisis survival skills as useful when pain is intense, cannot be solved quickly, and acting on emotions would make things worse.
The “10-minute rule” for emotional storms
Most emotional storms rise like a wave. They feel permanent, but they often peak and reduce if the person does not act immediately.
The patient can be taught:
“You do not have to solve your life now. You only have to postpone harmful action for 10 minutes.”
During those 10 minutes:
do not send the message,
do not cut,
do not drink,
do not drive,
do not make a relationship decision,
do not call repeatedly,
do not overdose,
do not threaten,
do not resign,
do not confront.
The aim is not to feel wonderful. The aim is to remain safe until the emotional wave drops by even 10–20%.
Skill 1: Feet-on-floor grounding
This is one of the simplest skills for panic, rage, dissociation, crying spells and self-harm urges.
Ask the patient to:
sit down,
place both feet firmly on the floor,
press the toes into the ground,
notice the pressure under the heels,
name the chair, room, date and place,
look around and say: “I am here, not there.”
This is useful because emotional storms often pull the person into memory, fear or imagined abandonment. Grounding brings the brain back to the present environment.
A simple script:
“Both feet on the floor. Back against the chair. Name five things you see. Name the place. Name today’s date. Say: this is an emotion, not an emergency.”
Skill 2: The 5–4–3–2–1 sensory method
This is easy to teach and easy to remember.
The patient names:
5 things they can see,
4 things they can feel,
3 things they can hear,
2 things they can smell,
1 thing they can taste.
This redirects attention from emotional rumination to sensory reality. It is especially useful for panic, dissociation, trauma activation and abandonment spirals.
It does not require belief. It only requires doing.
That is why it works well in the OPD population. Patients do not need to understand complex theory. They can start immediately.
Skill 3: Cold water and temperature shift
When emotion is extremely intense, cognitive skills may fail. Body-based skills are faster.
Cold water on the face, holding ice wrapped in cloth, or placing a cold pack near the cheeks can rapidly shift physiological arousal. In DBT, temperature change is part of the TIPP skill, used during extreme distress to bring down emotional intensity. DBT resources describe TIPP as a first-line crisis skill to reduce distress and prevent impulsive or harmful behaviours.
A practical version:
splash cold water on the face for 30 seconds,
hold ice wrapped in cloth,
place a cold pack on the face,
then sit and breathe slowly.
This is particularly useful when the patient says:
“I feel like cutting now.”
“I am going to explode.”
“I cannot stop crying.”
“I feel unreal.”
“I want to do something immediately.”
The cold sensation competes with the emotional surge and gives the brain a pause.
Skill 4: Paced breathing, not vague deep breathing
Many patients are told to “take deep breaths.” This can be too vague. Some patients overbreathe and feel worse.
Instead, teach a mechanical pattern:
inhale for 4 seconds,
exhale for 6 seconds,
repeat 10 times.
Or:
inhale 3,
exhale 5,
repeat for 2 minutes.
The key is a longer exhalation. This helps shift the body away from high arousal.
The instruction should be simple:
“Do not try to become peaceful. Just make the exhale longer than the inhale.”
This removes performance pressure.
Skill 5: Paired muscle relaxation
During intense emotion, the body becomes tight. The jaw, fists, shoulders, abdomen and legs may become tense.
A mechanical exercise:
tighten both fists for 5 seconds,
release for 10 seconds,
tighten shoulders for 5 seconds,
release for 10 seconds,
press feet into floor for 5 seconds,
release for 10 seconds.
Repeat three rounds.
This teaches the body the difference between tension and release. It is useful for anger, panic, self-harm urges and insomnia.
Skill 6: Intense but safe movement
Some emotions need movement before reflection.
For patients who become restless, agitated or self-harm driven, safe intense movement can help discharge arousal.
Examples:
fast walking for 10 minutes,
climbing stairs safely,
wall push-ups,
jumping jacks,
stationary cycling,
brisk walking inside the house,
carrying groceries,
cleaning a room.
The instruction:
“Move the body before you negotiate with the mind.”
This is not avoidance. It is nervous-system regulation.
Skill 7: The “do not text” rule
Many emotional crises worsen through the phone.
A patient may feel abandoned, angry or unsafe and send multiple messages. Later they feel ashamed, rejected or more dysregulated.
A practical OPD rule:
When emotion is above 7/10, do not send relationship messages.
Instead:
type it in Notes,
wait 30 minutes,
read it again,
send only if it is still wise,
or show it to therapist/doctor later.
A useful replacement message:
“I am emotionally overwhelmed now. I will respond later when I am calmer.”
This protects relationships.
For many EUPD/BPD patients, reducing crisis texting itself can reduce 30–40% of interpersonal damage.
Skill 8: Urge delay for self-harm
Self-harm urges are usually strongest when emotion feels unbearable. The first goal is to delay, not debate.
A patient can be taught:
delay for 10 minutes,
move away from sharp objects,
sit near another person if possible,
hold ice,
write the urge score,
call a support person,
use cold water,
walk,
repeat the delay.
The phrase:
“I am not promising never. I am postponing for 10 minutes.”
This is more acceptable to patients than “I will never self-harm again,” which may feel impossible during crisis.
DBT has evidence for reducing self-injury and suicidal behaviours in people with severe emotion dysregulation and borderline personality disorder.
Skill 9: The crisis card
Every patient with self-harm urges or intense emotional dysregulation should have a short crisis card.
It should fit on a phone note or small paper.
Example:
My warning signs:
rage, crying, urge to cut, urge to call repeatedly, feeling abandoned.
My first 3 skills:
cold water, feet on floor, 10-minute delay.
People I can contact:
one friend, one family member, doctor/emergency service.
Things I must not do for 30 minutes:
text, drink, cut, drive, threaten, resign, confront.
My reminder:
“This is a wave. I have survived this before.”
In crisis, memory collapses. A crisis card prevents the patient from needing to think from scratch.
Skill 10: Safe distraction
Distraction is often misunderstood. It is not denial. In crisis, safe distraction is a bridge.
Useful distractions:
fold clothes,
arrange books,
wash vessels,
take a shower,
walk outside safely,
watch a familiar comedy clip,
count backward from 100 by 7,
call someone and talk about neutral topics,
play a simple phone game for 10 minutes,
write the alphabet backward,
listen to one specific song playlist.
The key is to choose distractions before the crisis.
Do not ask the patient to invent coping skills while drowning.
Skill 11: Opposite action for emotional impulses
Once the crisis intensity reduces slightly, the patient can use emotion regulation skills.
If the urge is to isolate, take one small social step.
If the urge is to attack, speak slowly or leave the room.
If the urge is to self-harm, hold ice and contact support.
If the urge is to send a long angry message, send nothing or send one regulated line.
If the urge is to drink, eat, hydrate and leave the trigger place.
If the urge is to lie in bed all day, sit up and take a bath.
Opposite action does not mean pretending the emotion is absent. It means not obeying the emotion blindly.
Skill 12: Name the emotion accurately
Many patients say only: “I am feeling bad.”
But “bad” is too broad. Emotional regulation improves when the patient learns to name the state.
Is it anger?
shame?
fear?
abandonment?
jealousy?
guilt?
loneliness?
disappointment?
humiliation?
panic?
emptiness?
The psychiatrist can teach:
“Name it to tame it.”
For example:
“I am not dying. I am feeling abandoned.”
“I am not worthless. I am feeling shame.”
“I do not need to attack. I am feeling hurt.”
“I do not need to cut. I am feeling unbearable emotional pressure.”
This is a bridge from mechanical grounding to reflective therapy.
Skill 13: The traffic-light model
Patients often need a simple model.
Green zone: manageable
Emotion is 0–4/10.
Use journaling, therapy reflection, routine, exercise, problem-solving, communication skills.
Yellow zone: escalating
Emotion is 5–7/10.
Use grounding, paced breathing, walking, cold water, do-not-text rule, support call.
Red zone: crisis
Emotion is 8–10/10.
Do not problem-solve. Do not confront. Do not make decisions. Use crisis survival: cold water, remove means, contact support, emergency help if unsafe.
This helps patients understand that not every skill is for every moment.
Mindfulness and insight may work in green zone.
Grounding and distress tolerance are needed in yellow and red zones.
Why this approach works in OPD practice
In OPD settings, patients often cannot attend full DBT programmes immediately. They may have cost barriers, time limits, family resistance, crisis-driven visits or poor therapy access.
So the psychiatrist needs a practical first-aid model.
Early goals:
reduce self-harm,
reduce impulsive communication,
reduce alcohol/substance use during distress,
reduce emergency crises,
improve sleep,
increase follow-up,
build trust,
teach repeatable skills,
involve family when appropriate.
Once the patient becomes safer and more stable, deeper work can begin: mindfulness, trauma work, schema work, mentalisation, interpersonal patterns and identity development.
But safety comes first.
A suggested first-month plan for patients
Week 1: Safety and crisis map
Identify top three triggers.
Identify self-harm or impulsive behaviours.
Make a crisis card.
Teach cold water, grounding and 10-minute delay.
Remove or reduce access to means of self-harm.
Plan emergency contacts.
Week 2: Body regulation
Teach paced breathing.
Add walking or safe movement.
Fix sleep-wake routine.
Reduce alcohol and substance triggers.
Begin daily emotion rating from 0–10.
Week 3: Relationship protection
Introduce the do-not-text rule.
Teach “pause before reply.”
Write safe replacement messages.
Identify abandonment triggers.
Plan how to handle conflict without escalation.
Week 4: Relapse and self-harm prevention
Review what worked.
Identify crisis patterns.
Create a high-risk-day plan.
Add psychotherapy referral if feasible.
Treat comorbid depression, anxiety, ADHD, substance use or PMDD-like worsening when present.
This is simple, but it gives the patient a map.
What to tell patients who say “I cannot do mindfulness”
A helpful response is:
“You do not have to meditate perfectly. In the beginning, we are not aiming for enlightenment. We are aiming for safety. When emotions are very high, we will use body-based and grounding skills first. Once the storm reduces, mindfulness and deeper therapy will become easier.”
This reduces shame and increases engagement.
Many patients are relieved when they hear this. They stop feeling like they have failed therapy.
A simple OPD handout version
When emotion is above 7/10:
- Sit down. Feet on floor.
- Do not text, drink, cut, drive or confront for 10 minutes.
- Splash cold water or hold ice wrapped in cloth.
- Exhale longer than inhale for 2 minutes.
- Name five things you see.
- Move away from self-harm means.
- Write the message in Notes, not WhatsApp.
- Call one safe person.
- Repeat: “This is an emotion wave. I do not have to act now.”
- Seek urgent help if you cannot stay safe.
When urgent help is needed
Grounding skills are helpful, but they are not a substitute for emergency care.
Urgent psychiatric or emergency help is needed if there is:
active suicidal intent,
a plan to die,
recent serious self-harm,
overdose,
loss of control with violence,
severe intoxication,
psychosis,
inability to stay safe,
or no supportive person available during crisis.
The patient and family should be clearly told: skills are for surviving distress, not for silently enduring life-threatening risk.
Conclusion
Mindfulness is valuable, but it is not always the best first step for every patient. In early OPD care, many patients with emotional dysregulation, EUPD/BPD traits, trauma, panic, self-harm urges or intense relationship-triggered distress need mechanical, body-based, repeatable crisis skills first.
Grounding, cold water, paced breathing, movement, urge delay, crisis cards and relationship-protection rules can help patients survive emotional storms without making life worse.
Once the patient becomes safer, mindfulness becomes easier. Therapy becomes deeper. Insight becomes possible.
The sequence matters:
First safety.
Then stabilisation.
Then reflection.
Then deeper change.
That is often the most practical way to help patients move from emotional chaos to emotional regulation.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808