Catatonia
 Catatonia is one of the most striking syndromes in psychiatry—not merely because of its dramatic motor manifestations, but because it represents a profound disturbance at the interface of will, movement, and meaning. From its origins in classical German psychiatry to its modern reinterpretation as a transdiagnostic syndrome, catatonia has undergone a conceptual journey that mirrors the evolution of psychiatry itself.
Catatonia is one of the most striking syndromes in psychiatry—not merely because of its dramatic motor manifestations, but because it represents a profound disturbance at the interface of will, movement, and meaning. From its origins in classical German psychiatry to its modern reinterpretation as a transdiagnostic syndrome, catatonia has undergone a conceptual journey that mirrors the evolution of psychiatry itself.
To approach catatonia deeply is to ask:
What happens when the human capacity to initiate, modulate, and embody action begins to fragment?
🕰️ Historical Foundations: The German Psychopathological Tradition
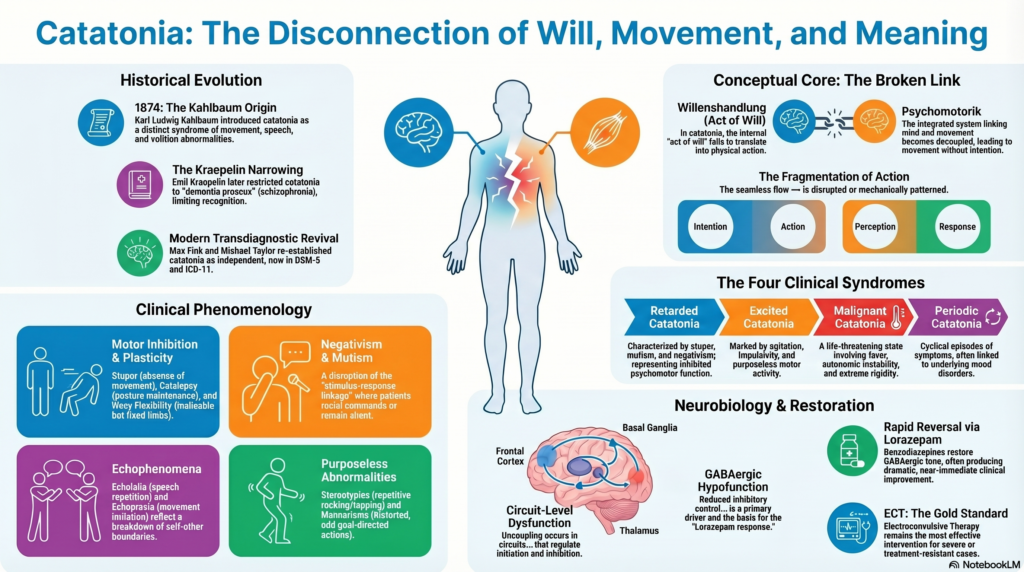
The term catatonia was introduced by Karl Ludwig Kahlbaum in 1874. Unlike later classifications, Kahlbaum described catatonia as a distinct syndrome characterized by abnormalities in movement, speech, affect, and volition, often evolving through phases.
His observations were grounded in the German tradition of careful phenomenology—where the aim was not merely classification, but faithful description of lived experience.
However, Emil Kraepelin later incorporated catatonia into dementia praecox, thereby restricting it to schizophrenia. This view persisted for decades, narrowing clinical recognition.
The revival of Kahlbaum’s broader vision came through the work of Max Fink and Michael Taylor, who re-established catatonia as a syndrome independent of diagnostic categories, now reflected in DSM-5 and ICD-11.
🧠 Conceptual Core: Disturbance of Will and Psychomotor Integration
At its essence, catatonia is a disorder of psychomotor integration—a failure in the seamless translation of:
- Intention → Action
- Perception → Response
- Affect → Expression
In classical German terminology, this can be framed as a disturbance of:
Willenshandlung (VIL-ens-hand-loong)
= “Act of will”
and
Psychomotorik (psy-cho-mo-TOH-rik)
= the integrated system linking mind and movement
In catatonia, these processes become decoupled.
The patient may:
- Have intention but no movement
- Exhibit movement without intention
- Respond in ways that are mechanically patterned but experientially disconnected
📋 Clinical Phenomenology with German Concepts
Catatonia is best understood not as isolated signs, but as expressions of altered motor intentionality.
⚡ I. Motor Inhibition and Plasticity
Stupor (Stupor — SHTOO-por)
A state of near-complete absence of movement and responsiveness.
- Consciousness may be preserved
- The patient appears frozen in existence
This reflects a profound inhibition of Willenshandlung—the will cannot translate into action.
Catalepsy (Katalepsie — ka-ta-LEP-see)
Passive maintenance of imposed posture.
- Limbs remain where placed
- Suggests altered motor regulation
Waxy Flexibility (Cerea flexibilitas — SEH-ray-ah fleks-ih-bil-ih-tas)
A mild, even resistance to movement followed by maintenance of posture.
- The body behaves like soft wax
- Malleable, yet fixed
In German descriptions, this reflects a peculiar plasticity of motor tone—neither rigid nor relaxed.
⚡ II. Negativism and Mutism
Mutism (Mutismus — MOO-tis-moos)
Marked reduction or absence of speech.
- Not due to aphasia
- Reflects withdrawal of expressive function
Negativism (Negativismus — neh-ga-TEE-vis-moos)
Opposition or absence of response to external stimuli.
- Active: resisting commands
- Passive: failure to respond
This is not mere defiance. It represents a disruption in:
Reiz-Reaktions-Verbindung (RYTES-reh-ak-tsi-ONS-fer-BIN-doong)
= stimulus-response linkage
The patient is no longer able to translate external input into adaptive action.
⚡ III. Motor Abnormalities
Posturing (Haltungsstereotypien — HAL-toongs-shteh-reh-oh-tee-pee-en)
Spontaneous maintenance of abnormal postures.
- Often prolonged
- May appear symbolic
Stereotypies (Stereotypien — shteh-reh-oh-tee-PEE-en)
Repetitive, non-goal-directed movements.
- Rocking, tapping
Represent motor output detached from purpose.
Mannerisms (Manierismen — ma-NEER-is-men)
Distorted, exaggerated versions of normal actions.
- Goal-directed but odd
Grimacing (Grimassieren — gri-MAS-see-ren)
Persistent abnormal facial expressions.
⚡ IV. Echophenomena
Echolalia (Echolalie — ek-oh-la-LEE)
Repetition of speech
Echopraxia (Echopraxie — ek-oh-prak-SEE)
Imitation of movements
These reflect a disturbance in self-other boundaries at the motor level, where external actions are mirrored without internal modulation.
⚡ V. Excited Catatonia
Agitation (Erregung — eh-REG-oong)
Excessive, purposeless motor activity.
- Not influenced by external stimuli
- May alternate with stupor
This paradox—immobility and hyperactivity coexisting—is central to catatonia.
⚡ Catatonia Syndromes (Fink & Taylor Framework)
Max Fink and Michael Taylor described distinct clinical syndromes:
Retarded Catatonia
- Stupor, mutism, negativism
- Represents inhibition of psychomotor function
Excited Catatonia
- Agitation, impulsivity
- Represents disinhibited motor output
Malignant Catatonia
- Fever, autonomic instability, rigidity
- Life-threatening
Periodic Catatonia
- Cyclical episodes
- Often linked to mood disorders
🔬 Neurobiology: A Systems Perspective
Catatonia reflects dysfunction across multiple systems:
1. GABAergic Hypofunction
- Basis for response to Lorazepam
- Reduced inhibitory control
2. Glutamatergic Dysregulation
- NMDA receptor involvement
3. Dopaminergic Dysfunction
- Particularly in malignant catatonia
4. Circuit-Level Dysfunction
Catatonia can be conceptualized as a disorder of distributed neural circuits rather than a lesion in a single structure. The dysfunction primarily involves an integrated network linking the:
- Frontal cortex (especially medial and dorsolateral regions)
- Basal ganglia (striatum and related nuclei)
- Thalamus
Together, these structures form fronto–striato–thalamo–cortical loops, which are essential for the seamless orchestration of behavior.
Under normal conditions, these circuits subserve three fundamental operations:
- Initiation — the generation of action from intention
- Inhibition — the suppression of irrelevant or competing responses
- Modulation — the fine-tuning, sequencing, and contextual adaptation of movement
In catatonia, these processes do not simply fail—they become functionally decoupled.
- Intentions may arise but fail to translate into movement (stupor)
- Motor output may occur without appropriate inhibitory control (agitation, stereotypies)
- Actions, when present, lose their contextual coherence and adaptive modulation
Thus, catatonia reflects not merely hypo- or hyperactivity of motor systems, but a deeper disturbance in the integration of volition, control, and execution—a failure of the brain’s capacity to align will, movement, and meaning into a coherent behavioral act.
💊 Therapeutic Evolution: From ECT to Lorazepam
Historically, catatonia was treated with Electroconvulsive Therapy (ECT).
- Rapid, effective
- Still gold standard in severe cases
The discovery of the lorazepam response transformed practice:
- Benzodiazepines restore GABAergic tone
- Often produce dramatic, near-immediate improvement
This shift marked a key transition:
From a purely somatic intervention (ECT) to a neurochemical understanding of catatonia.
🧭 Contemporary Perspective
Catatonia is now understood as:
- Transdiagnostic
- Common but under-recognized
- Highly treatable
Seen in:
- Mood disorders (especially bipolar disorder)
- Medical conditions
- Substance-related states
No longer confined to schizophrenia.
🧩 Closing Reflection
Catatonia challenges our assumptions about movement and will.
It reveals that:
- Action is not merely voluntary
- Speech is not merely expressive
- Movement is not merely mechanical
All are embedded in delicate systems integrating mind, brain, and body.
In catatonia, this integration fails.
The patient may appear silent, immobile, or chaotic—but beneath this lies a deeper disturbance:
A disconnection between intention and execution,
between inner life and outward expression.
And yet, unlike many psychiatric syndromes, catatonia offers something rare:
The possibility of rapid reversal—if recognized in time.
📘 About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808