Tics in OCD Patients: Understanding the Overlap, the Clues, and the Clinical Approach
 The relationship between Obsessive-Compulsive Disorder (OCD) and tics is one of the most clinically important—and often under-recognized—areas in psychiatry.
The relationship between Obsessive-Compulsive Disorder (OCD) and tics is one of the most clinically important—and often under-recognized—areas in psychiatry.
Many patients with OCD, especially younger males, present with:
- Repetitive movements
- Urges to perform actions “just right”
- Sudden, non-purposeful behaviors
These are often misinterpreted as compulsions.
But in a significant subset, they are actually tics.
Understanding this distinction can change diagnosis, prognosis, and treatment.
What are Tics?
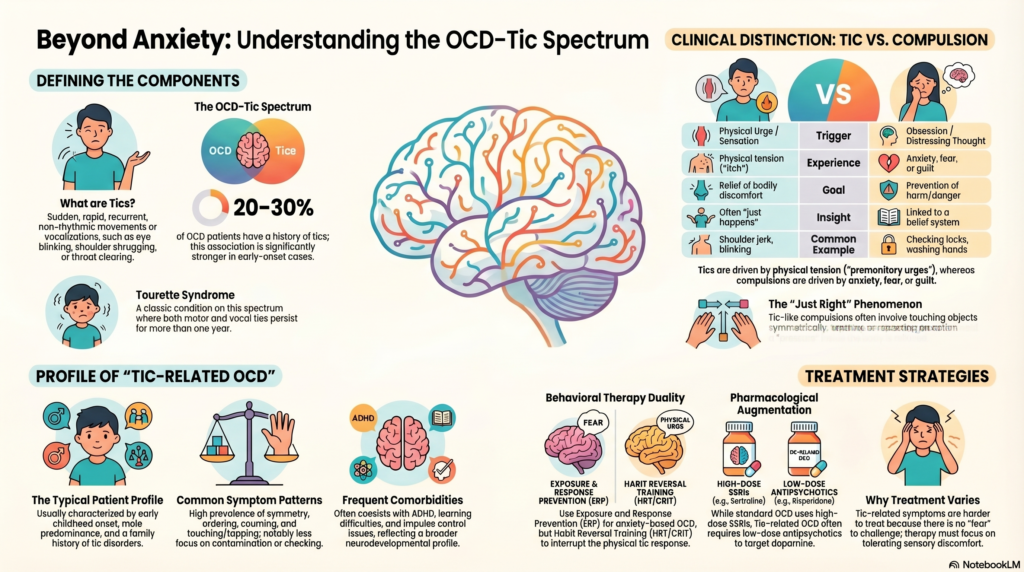
Tics are sudden, rapid, recurrent, non-rhythmic motor movements or vocalizations.
They are broadly classified into:
Motor Tics
- Eye blinking
- Facial grimacing
- Shoulder shrugging
- Head jerking
Vocal (Phonic) Tics
- Throat clearing
- Sniffing
- Grunting
- Repetition of sounds/words
A classic condition is Tourette syndrome, where both motor and vocal tics are present for more than a year.
The OCD–Tic Spectrum
OCD and tic disorders are not separate silos—they exist on a neurodevelopmental spectrum.
In fact:
- Around 20–30% of OCD patients have current or past tics
- The association is stronger in early-onset OCD
This subtype is often called:
➡️ Tic-related OCD
Why This Overlap Happens
Both OCD and tics share dysfunction in:
- Cortico-striato-thalamo-cortical (CSTC) circuits
- Particularly involving:
- Basal ganglia
- Orbitofrontal cortex
- Anterior cingulate
This explains why:
- Some compulsions look like tics
- Some tics feel like compulsions
Key Clinical Distinction: Tic vs Compulsion
This is where clinical skill matters.
| Feature | Tic | Compulsion |
|---|---|---|
| Trigger | Urge / sensation | Obsession / thought |
| Experience | Physical tension (“premonitory urge”) | Anxiety, fear, guilt |
| Goal | Relief of bodily discomfort | Prevention of harm |
| Insight | Often “just happens” | Linked to belief system |
| Example | Shoulder jerk | Checking lock repeatedly |
The Premonitory Urge (Core Concept)
Patients with tics often describe:
- “A pressure builds up”
- “An itch inside the body”
- “I have to do it to feel relief”
This is not anxiety-driven—it is sensorimotor.
This is the most important differentiator.
When OCD and Tics Mix
In many patients, especially adolescents:
- Tics and compulsions coexist
- Or merge into “tic-like compulsions”
Examples:
- Repeating an action until it feels “just right”
- Touching objects symmetrically
- Blinking or breathing rituals
These are often not driven by fear of harm, but by:
➡️ A need for sensory completeness
Clinical Subtype: Tic-Related OCD
This subtype has distinct features:
Typical Profile:
- Early onset (childhood/adolescence)
- Male predominance
- Family history of tics
- More “just right” phenomena
- Less elaborate obsessional fears
Symptom Pattern:
- Symmetry, ordering, repetition
- Touching, tapping
- Counting behaviors
- Less contamination or checking (classically)
Important Comorbidities
Tic-related OCD often coexists with:
- Attention Deficit Hyperactivity Disorder
- Learning difficulties
- Impulse control issues
This cluster reflects a neurodevelopmental profile, rather than purely anxiety-driven OCD.
Why This Matters Clinically
Misidentifying tics as compulsions can lead to:
- Over-reliance on cognitive therapy alone
- Poor response to standard OCD treatment
- Frustration for both patient and clinician
Recognizing tics allows for:
➡️ More precise, tailored treatment
Treatment Approach
1. Behavioral Therapy
For OCD:
- Exposure and Response Prevention (ERP)
For Tics:
- Habit Reversal Training (HRT) / CBIT (Comprehensive Behavioral Intervention for Tics)
Key difference:
- ERP → tolerate anxiety
- HRT → interrupt the tic response using competing actions
2. Pharmacological Treatment
OCD:
- SSRIs (high dose)
Tic-related OCD:
Often requires augmentation:
- Antipsychotics (low dose):
- Risperidone
- Aripiprazole
These target dopaminergic dysregulation seen in tic circuits.
3. Addressing the “Just Right” Phenomenon
These symptoms are harder to treat because:
- No clear fear to challenge
- Driven by internal discomfort
Approach:
- Gradual exposure to incomplete actions
- Tolerating sensory discomfort
- Reducing repetition
A Subtle Clinical Insight
Patients with tic-related OCD often say:
- “It doesn’t feel right unless I do it”
- “I don’t know why I’m doing it—it just bothers me if I don’t”
This reflects a shift:
From fear-driven OCD → to urge-driven behavior
Understanding this changes how we frame therapy.
Prognosis
- Tic-related OCD tends to be more chronic
- May respond less robustly to SSRIs alone
- But improves significantly with:
- Combined behavioral approaches
- Appropriate pharmacological augmentation
Final Reflection
Not every repetitive act in OCD is a compulsion.
Some are driven not by fear—but by the body’s urge for completion.
When we recognize this distinction,
we move from treating “anxiety” alone
to treating the underlying neurobehavioral circuitry.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist
Apollo Clinic Velachery (Opp. Phoenix Mall)
Special interest in OCD spectrum disorders, tic disorders, and neurodevelopmental psychiatry, integrating ERP, CBIT, and objective tools like QEEG and computerized assessments.
📞 +91-8595155808
✉ srinivasaiims@gmail.com