Theta Burst Stimulation, the Default Mode Network, and the Neuroscience of Placebo Response in Depression
 A recent JAMA Psychiatry randomized clinical trial by Snyder, Handoko, Neppach, et al. explores a fascinating question in modern psychiatry: can brain stimulation amplify the antidepressant placebo effect by modulating the default mode network? The study examined whether intermittent theta burst stimulation over the dorsomedial prefrontal cortex could enhance the way treatment expectancy translates into mood improvement.
A recent JAMA Psychiatry randomized clinical trial by Snyder, Handoko, Neppach, et al. explores a fascinating question in modern psychiatry: can brain stimulation amplify the antidepressant placebo effect by modulating the default mode network? The study examined whether intermittent theta burst stimulation over the dorsomedial prefrontal cortex could enhance the way treatment expectancy translates into mood improvement.
This is not merely a paper about placebo. It is a paper about expectation, prediction, meaning, brain networks, and the biology of hope.
The Big Question
In clinical trials, placebo is often treated as a nuisance — something to subtract from the “real” drug effect. But in psychiatry, placebo response is not simply fake improvement. It is a genuine psychobiological response shaped by:
- expectation,
- learning,
- therapeutic context,
- trust,
- prior treatment experience,
- prediction,
- emotional meaning.
The authors ask whether these expectancy-driven mood effects can be experimentally enhanced using neuromodulation.
Their central question was:
Can stimulation of the dorsomedial prefrontal cortex modulate default mode network activity and thereby strengthen placebo-induced mood improvement?
The answer, cautiously, appears to be yes.
Why the Default Mode Network Matters
The default mode network, or DMN, is a large-scale brain network involved in:
| DMN Function | Clinical Relevance |
|---|---|
| Self-referential thinking | “What does this mean for me?” |
| Future simulation | “Will I get better?” |
| Autobiographical memory | Linking present experience with past treatment experiences |
| Emotional appraisal | Giving affective meaning to events |
| Internal prediction | Constructing expectations about the future |
In depression, the DMN is often associated with rumination, negative self-focus, hopelessness, and repetitive internal narratives. But this study reminds us that the DMN is not merely a “depression network.” It is also a meaning-making network.
The same system that can trap a patient in negative self-reflection may also help convert hope into emotional change when modulated appropriately.
Study Design in Simple Terms
The researchers conducted a within-person, counterbalanced randomized clinical trial. Adults with depressive symptoms, who were not taking psychotropic medication, underwent three stimulation conditions:
| Condition | Meaning |
|---|---|
| iTBS | Intermittent theta burst stimulation; expected to have potentiating/excitatory-like effects |
| cTBS | Continuous theta burst stimulation; expected to have depotentiating/inhibitory-like effects |
| sTBS | Sham theta burst stimulation; control condition |
The stimulation target was the dorsomedial prefrontal cortex, localized around EEG coordinate F2, at 80% resting motor threshold. Sessions were one week apart. About one hour after stimulation, participants completed an antidepressant placebo fMRI task that manipulated treatment expectancy using cues and sham neurofeedback.
The final analytic sample included 50 participants, with a mean age of approximately 28 years.
What Was the Placebo Task?
Participants were told a cover story involving a fast-acting versus conventional intravenous antidepressant. During fMRI, they saw expectancy cues and received sham neurofeedback. They then rated their expectancy and mood.
The task was designed to examine how the brain responds when a person believes that a treatment may improve their mood.
This makes the study highly relevant to psychiatry because much of psychiatric treatment depends not only on the biological action of medication or stimulation, but also on how patients understand, anticipate, and emotionally register treatment.
Main Finding: iTBS Increased DMN Activation
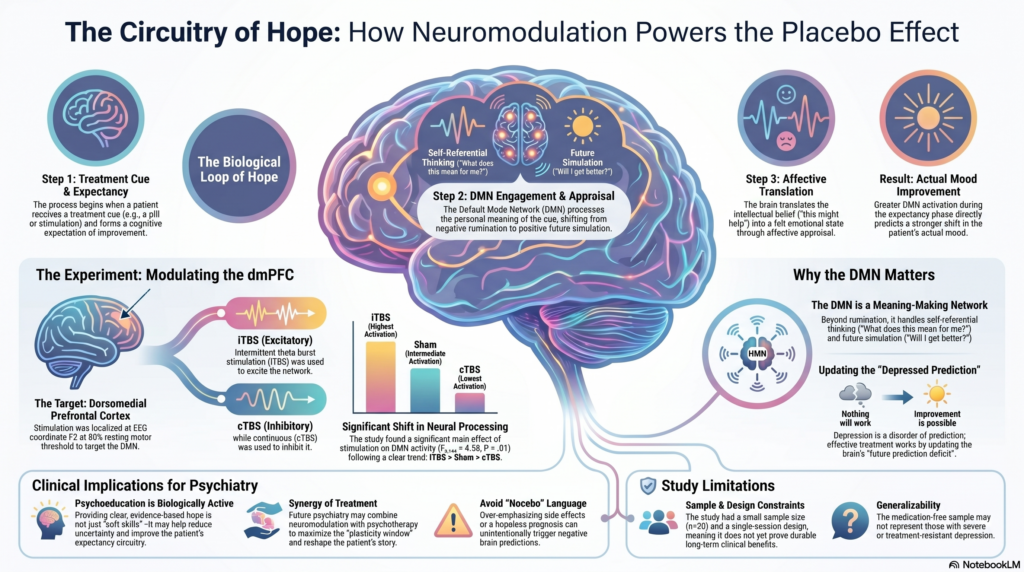
The key result was that intermittent theta burst stimulation increased DMN activation during expectancy processing compared with continuous theta burst stimulation.
The pattern was:
iTBS > sham TBS > cTBS
This is beautifully shown in the uploaded Figure 2. The brain maps show increased DMN BOLD activation during expectancy processing, while the box plot shows a graded pattern across stimulation conditions: lowest with cTBS, intermediate with sham, and highest with iTBS.
The authors reported a significant main effect of stimulation condition on DMN activity:
F₂,₁₄₄ = 4.55; P = .01; η² = 0.06
They also found a significant monotonic trend:
iTBS > sTBS > cTBS
This suggests that theta burst stimulation can experimentally shift the neural processing of expectancy.
The Most Important Finding: Expectancy Became Mood
The most clinically interesting finding was not simply that iTBS activated the DMN. It was that greater DMN activation under iTBS predicted stronger expectancy-related mood improvement.
In other words:
When the DMN was potentiated, positive expectation was more likely to become actual mood improvement.
This is a crucial distinction.
A patient may intellectually believe, “This treatment may help me.”
But the deeper therapeutic question is:
Does that belief become emotionally felt?
This study suggests that the DMN may be one of the brain systems through which expectancy is translated into affective change.
Scientific Interpretation
The study supports a model in which placebo response in depression involves a loop:
treatment cue → expectancy → salience processing → DMN engagement → affective appraisal → mood improvement
The salience network may identify the treatment cue as important. The dorsal attention network may help orient attention to treatment-related signals. But the default mode network may give those signals personal meaning.
This matters because depression is not only low mood. It is also a disorder of prediction.
The depressed brain often predicts:
- “Nothing will change.”
- “Treatment will not work.”
- “I will remain this way.”
- “My future is closed.”
Effective treatment may partly work by updating these predictions. Medication, psychotherapy, neuromodulation, and therapeutic alliance may all act, in different ways, on the patient’s predictive model of self and future.
Why This Paper Is Conceptually Important
This paper moves psychiatry beyond a simplistic model:
drug → receptor → symptom improvement
Toward a richer model:
treatment context → expectancy → brain network modulation → emotional change
This does not reduce psychiatry to placebo. Rather, it shows that expectancy is one component of treatment biology.
In clinical practice, this means the psychiatrist’s words, explanations, confidence, clarity, and therapeutic framing are not merely “soft skills.” They may influence measurable brain mechanisms.
Placebo Is Not Fake
A major takeaway from this study is that placebo response should not be dismissed as imaginary.
Placebo effects involve real brain processes, including networks responsible for:
- valuation,
- affective appraisal,
- reinforcement learning,
- prediction,
- interoception,
- self-referential meaning.
In depression, hope is not just a poetic idea. It may be a neural process.
The ethical clinical goal is not to deceive patients. The goal is to create truthful, evidence-based, credible hope.
A clinician saying:
“This treatment has evidence, we will monitor your progress carefully, and there are several steps we can take if this does not work”
is not merely giving reassurance. That statement may reduce uncertainty, enhance agency, and improve the patient’s expectancy system.
Clinical Relevance for Psychiatry
The study has several implications for everyday psychiatric practice.
1. Psychoeducation is biologically active
When patients understand their illness and treatment, they are more likely to engage meaningfully. Good psychoeducation may reduce fear and improve expectancy.
2. Therapeutic alliance matters
Trust is not decorative. It may shape the brain’s response to treatment.
3. Nocebo language should be avoided
Excessive emphasis on side effects, hopeless prognosis, or chronicity may unintentionally worsen negative expectations.
4. Neuromodulation and psychotherapy may be synergistic
A future direction could be combining TBS with structured psychotherapy during the post-stimulation plasticity window.
5. Depression treatment may need prediction updating
Patients with depression often struggle not only with mood but with the inability to imagine improvement. Treatment must target this “future prediction deficit.”
Important Limitations
This study is scientifically exciting, but it should not be overinterpreted.
It does not mean that iTBS should now be used clinically to “boost placebo response.”
Key limitations include:
| Limitation | Why It Matters |
|---|---|
| Final sample size of 50 | Small for complex neuroimaging and neuromodulation modelling |
| Single-session design | Does not prove durable clinical antidepressant benefit |
| Medication-free sample | May not generalize to severe or treatment-resistant depression |
| Depressive symptoms, not necessarily all MDD | Findings may differ in syndromal major depressive disorder |
| Scalp-based targeting | Less precise than MRI-guided neuronavigation |
| No individual electric-field modelling | Actual stimulation dose may vary between individuals |
| Placebo deception paradigm | Not directly transferable to routine ethical clinical care |
| BOLD fMRI outcome | Indirect measure of neural activity |
The authors themselves conclude that repeated protocols, larger samples, more severe clinical populations, and integration with pharmacological and psychotherapeutic interventions need further study before clinical translation.
A Psychiatrist’s Reading
This paper is important because it separates two processes:
expecting improvement
and
emotionally experiencing improvement
Many patients say:
“I know the treatment should help, but I don’t feel it.”
This study suggests that the gap between cognitive belief and emotional change may be mediated by brain networks such as the DMN, especially medial prefrontal and cingulate regions involved in self-appraisal and affective prediction.
For psychiatry, this opens an exciting future: treatment may not only involve correcting neurotransmitters, but also reshaping the patient’s predictive relationship with the future.
Final Takeaway
This JAMA Psychiatry trial suggests that intermittent theta burst stimulation of the dorsomedial prefrontal cortex can potentiate default mode network activity and strengthen the conversion of antidepressant expectancy into mood improvement.
The larger message is profound:
Hope is not merely psychological. Hope has circuitry.
Modern psychiatry must learn to work at both levels — the synapse and the story, the circuit and the meaning, the molecule and the expectation.
Detailed Citation
Snyder I, Handoko K, Neppach A, et al. Intermittent Theta Burst Stimulation of the Dorsomedial PFC and Expectancy-Driven Placebo Mood Effects: A Randomized Clinical Trial. JAMA Psychiatry. Published online May 6, 2026. doi: 10.1001/jamapsychiatry.2026.0647.
Article link: JAMA Psychiatry article
DOI link: https://doi.org/10.1001/jamapsychiatry.2026.0647
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808