SAINT and Related Accelerated rTMS Protocols: The Future of Rapid-Acting Neuromodulation in Depression
 For decades, depression treatment has largely followed a slow clinical rhythm: start an antidepressant, wait weeks, increase the dose, switch, augment, and wait again. This approach works for many patients, but for those with treatment-resistant depression, the waiting itself can become part of the illness. Persistent low mood, suicidal ideation, cognitive slowing, insomnia, anhedonia, and loss of agency demand treatments that are not only effective, but also faster.
For decades, depression treatment has largely followed a slow clinical rhythm: start an antidepressant, wait weeks, increase the dose, switch, augment, and wait again. This approach works for many patients, but for those with treatment-resistant depression, the waiting itself can become part of the illness. Persistent low mood, suicidal ideation, cognitive slowing, insomnia, anhedonia, and loss of agency demand treatments that are not only effective, but also faster.
This is where accelerated repetitive transcranial magnetic stimulation, especially Stanford Accelerated Intelligent Neuromodulation Therapy — SAINT, enters the field.
What is rTMS?
Repetitive transcranial magnetic stimulation, or rTMS, is a non-invasive brain stimulation technique in which rapidly changing magnetic fields are used to modulate cortical activity. In depression, the most common target is the left dorsolateral prefrontal cortex, a region involved in executive control, emotional regulation, motivation, and top-down modulation of limbic circuits.
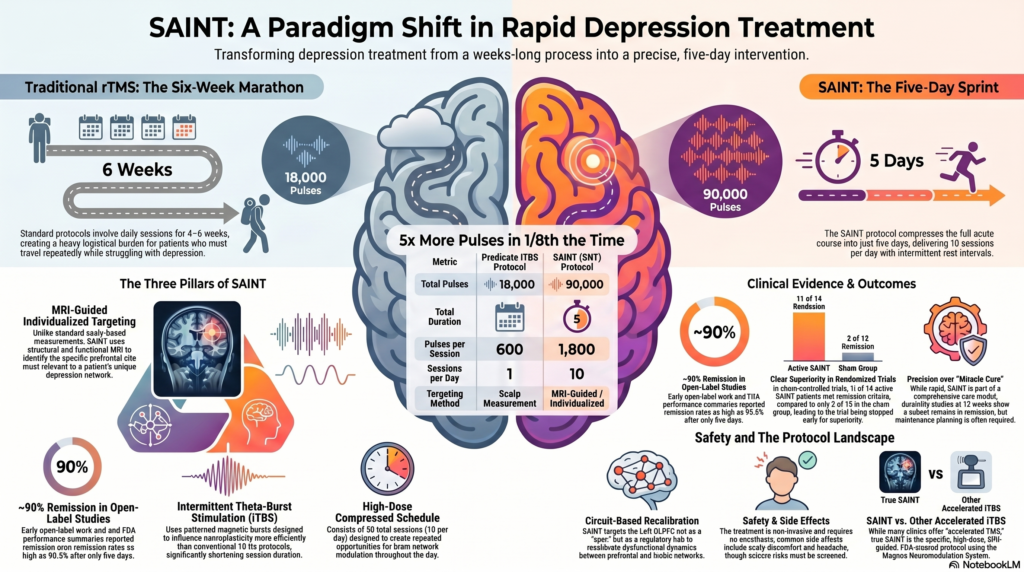
Traditional rTMS for depression usually involves daily sessions over four to six weeks. This is effective for many patients, but the treatment burden is substantial. Patients must travel repeatedly, arrange work schedules, and sustain motivation despite depressive symptoms. Accelerated protocols attempt to solve this problem by compressing treatment into fewer days without simply “rushing” the science.
What is SAINT?
SAINT, now often referred to in the literature as Stanford Neuromodulation Therapy — SNT, is a precision accelerated neuromodulation protocol developed at Stanford. It is not just “more TMS in fewer days.” It combines three key elements:
First, it uses MRI-guided individualised targeting. Instead of relying only on scalp measurements, SAINT uses structural and functional MRI data to identify a personalised target within the left dorsolateral prefrontal cortex. The aim is to stimulate a prefrontal site most relevant to the patient’s depression network. The FDA summary describes the system as using structural and functional MRI data, neuronavigation, motor-threshold determination, and patient-specific targeting within the left DLPFC.
Second, it uses intermittent theta-burst stimulation, or iTBS. Theta-burst stimulation delivers patterned bursts designed to influence neuroplasticity more efficiently than older conventional protocols. In standard clinical research, iTBS has shown non-inferior antidepressant outcomes compared with conventional 10 Hz rTMS, with much shorter session duration.
Third, SAINT uses a high-dose compressed schedule. The FDA-cleared Magnus Neuromodulation System with SAINT Technology delivers 1,800 pulses per session, 10 sessions per day, 50 total sessions, and 90,000 pulses over five days. This is compared with the predicate iTBS protocol of 600 pulses per session and 18,000 total pulses over six weeks.
The five-day depression treatment model
The headline feature of SAINT is speed. A full acute course is completed in five days, typically with 10 treatment sessions per day. Each session is separated by rest intervals. This high-dose, spaced stimulation model is designed to create repeated opportunities for network modulation across the day.
This matters clinically because depression is not merely sadness. It is a disorder of mood, cognition, reward, bodily energy, sleep, self-evaluation, and future expectation. A treatment that can produce meaningful improvement within days rather than weeks has major implications for patients who are severely impaired, occupationally disabled, or losing hope.
Evidence: promising, but should be presented carefully
SAINT/SNT has generated remarkable early results, but it should be discussed with scientific caution.
Early open-label work reported remission rates approaching 90% after five days. The FDA performance summary also cites an open-label SAINT study in which 19 of 21 participants, or 90.5%, met remission criteria based on MADRS.
The more important evidence comes from the sham-controlled randomized trial. In that study, the FDA summary reports that 11 of 14 patients receiving active SAINT met remission criteria, compared with 2 of 15 in the sham group. Response was seen in 12 of 14 active-treatment patients, compared with 4 of 15 in the sham group. The trial was stopped early because of clear superiority of active treatment.
Therefore, the most accurate wording is not:
“SAINT guarantees 90% remission.”
A more responsible statement is:
“SAINT/SNT has shown unusually rapid and high remission rates in treatment-resistant depression, with early open-label studies reporting around 90% remission and controlled trial data showing strong superiority over sham treatment.”
FDA-cleared, not just experimental
The Magnus Neuromodulation System with SAINT Technology received FDA 510(k) clearance for the treatment of major depressive disorder in adult patients who have failed to achieve satisfactory improvement from antidepressant medication in the current episode.
This distinction matters. SAINT is not merely a theoretical research protocol. However, the cleared system is specific: it involves the device ecosystem, MRI-informed targeting, neuronavigation, and the five-day accelerated iTBS protocol. Not every clinic offering “accelerated TMS” is offering true SAINT.
Why SAINT is conceptually important
The deeper importance of SAINT is that it reflects a shift in psychiatry: from symptom-based treatment to circuit-based treatment.
Depression can be understood as a disorder of disrupted communication between prefrontal control networks, limbic affective systems, salience networks, default mode networks, and reward circuits. The left DLPFC is not stimulated because it is a “depression spot.” It is targeted because it is a regulatory hub capable of influencing distributed mood networks.
In this model, neuromodulation is not simply “activating the brain.” It is an attempt to recalibrate dysfunctional network dynamics.
Related protocol 1: Conventional 10 Hz left DLPFC rTMS
The older and still widely used protocol is high-frequency 10 Hz rTMS to the left DLPFC, usually delivered over four to six weeks. It remains a well-established treatment option for depression, especially when antidepressants have not produced adequate benefit.
Its advantage is that it has a broad evidence base and is widely available. Its limitation is logistical burden. Patients need many visits, and improvement may take weeks.
Related protocol 2: Intermittent theta-burst stimulation
Intermittent theta-burst stimulation, or iTBS, is a shorter stimulation pattern that can be delivered in a few minutes. The major THREE-D trial showed that iTBS was non-inferior to conventional 10 Hz rTMS for treatment-resistant depression, with similar tolerability. This established iTBS as a major step forward because it reduced treatment time without clearly sacrificing efficacy.
In practical terms, iTBS made TMS more scalable. More patients can be treated in a day, treatment burden is reduced, and clinics can potentially deliver neuromodulation more efficiently.
Related protocol 3: Accelerated iTBS without full SAINT targeting
Many centres and researchers have explored accelerated iTBS, where multiple iTBS sessions are given per day over several days. These protocols may resemble SAINT in schedule, but they may not use the same MRI-guided personalised targeting or proprietary dosing structure.
This is an important distinction. Accelerated iTBS is a family of approaches. SAINT/SNT is a specific, high-dose, MRI-guided, FDA-cleared version within that family.
A 2024 systematic review and network meta-analysis of theta-burst stimulation for depression included 23 randomized controlled trials and 960 participants, showing the growing evidence base for TBS approaches, though protocols vary considerably across studies.
Related protocol 4: Bilateral theta-burst stimulation
Some depression protocols use bilateral stimulation: excitatory stimulation to the left DLPFC and inhibitory stimulation to the right DLPFC. This is based on the idea that depression may involve relative underactivity of left prefrontal regulatory systems and overactivity or maladaptive activity in right prefrontal networks.
In older adults with treatment-resistant depression, a randomized noninferiority trial found that bilateral theta-burst stimulation was non-inferior to standard bilateral rTMS, while taking only about four minutes compared with a much longer standard bilateral session.
This is clinically relevant for geriatric depression, where treatment tolerability, cognitive safety, travel burden, and medical comorbidity are major considerations.
Related protocol 5: Deep TMS and other device-based approaches
Deep TMS uses different coil designs to reach broader or deeper cortical-subcortical networks. It has FDA-cleared indications for depression and some other conditions depending on jurisdiction and device. It is not the same as SAINT. Deep TMS focuses more on coil geometry and field distribution, whereas SAINT’s uniqueness lies in functional MRI-guided personalised targeting and a compressed high-dose iTBS schedule.
Durability: the key unanswered question
The biggest question is not only whether SAINT works rapidly, but how long the benefit lasts after a single five-day course.
A 2025 durability study concluded that at 12 weeks, a subset of participants remained in remission, but durability requires further study.
This is clinically important. Depression is often a relapsing-remitting disorder. Even if rapid remission occurs, many patients may still require maintenance planning: medication optimization, psychotherapy, relapse prevention, sleep stabilization, lifestyle work, booster neuromodulation sessions, or treatment of comorbid anxiety, substance use, ADHD, trauma, or personality vulnerabilities.
Safety and clinical caution
rTMS and iTBS are generally non-invasive and do not require anesthesia. Common side effects include scalp discomfort and headache. Serious adverse events such as seizures are rare but must be actively screened for. Patients require evaluation for seizure risk, implanted metallic or electronic devices, bipolar disorder, psychosis, substance use, unstable medical conditions, and medications that may lower seizure threshold.
SAINT should not be marketed as a miracle cure. It is best framed as a rapid, evidence-based, precision neuromodulation option for appropriately selected patients with major depression who have not responded adequately to medication.
SAINT is not a replacement for all depression treatments
SAINT may be especially useful for treatment-resistant depression where speed matters, but it does not eliminate the need for comprehensive psychiatric care. Depression may be maintained by biological vulnerability, sleep disruption, grief, trauma, interpersonal stress, addiction, endocrine disease, chronic pain, neurodegeneration, or psychosocial adversity.
Neuromodulation can open the door. Psychotherapy, medication, family work, behavioural activation, and relapse prevention help the patient walk through it.
The future: precision psychiatry
SAINT represents the direction in which psychiatry is moving. The future will likely involve:
- MRI-guided and EEG-guided targeting
- symptom-network-based protocols
- personalization based on connectivity patterns
- accelerated schedules for rapid relief
- maintenance protocols based on relapse prediction
- integration with psychotherapy and digital monitoring
The broader message is powerful: depression is not a weakness of character. It is a modifiable brain-network disorder. When treatment is targeted precisely, the brain may recover faster than we previously imagined.
Conclusion
SAINT and related accelerated rTMS protocols mark an important transition in depression care. Conventional antidepressants remain important. Psychotherapy remains important. ECT and ketamine remain important for selected patients. But accelerated neuromodulation adds something new: the possibility of rapid, non-invasive, circuit-based treatment for severe and treatment-resistant depression.
The responsible clinical stance is neither hype nor dismissal. SAINT is not magic. But it is one of the most exciting developments in modern biological psychiatry — a sign that the field is moving from trial-and-error prescribing toward personalised brain-network therapeutics.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery, Chennai
✉ srinivasaiims@gmail.com 📞 +91-8595155808