CBT-ED: The Modern Cognitive Behavioural Approach to Eating Disorders
 Eating disorders are not simply problems of “food” or “willpower.” They are complex psychiatric conditions where eating, weight, body image, fear, shame, control, emotion regulation, and identity become deeply entangled. Disorders such as anorexia nervosa, bulimia nervosa, binge-eating disorder, OSFED, and ARFID can cause severe psychological distress, medical complications, functional impairment, and even increased mortality. Among the available psychological treatments, Cognitive Behavioural Therapy for Eating Disorders — CBT-ED — remains one of the strongest evidence-based approaches, but recent research also reminds us that it needs to become faster, more accessible, more personalised, and more developmentally sensitive.
Eating disorders are not simply problems of “food” or “willpower.” They are complex psychiatric conditions where eating, weight, body image, fear, shame, control, emotion regulation, and identity become deeply entangled. Disorders such as anorexia nervosa, bulimia nervosa, binge-eating disorder, OSFED, and ARFID can cause severe psychological distress, medical complications, functional impairment, and even increased mortality. Among the available psychological treatments, Cognitive Behavioural Therapy for Eating Disorders — CBT-ED — remains one of the strongest evidence-based approaches, but recent research also reminds us that it needs to become faster, more accessible, more personalised, and more developmentally sensitive.
What is CBT-ED?
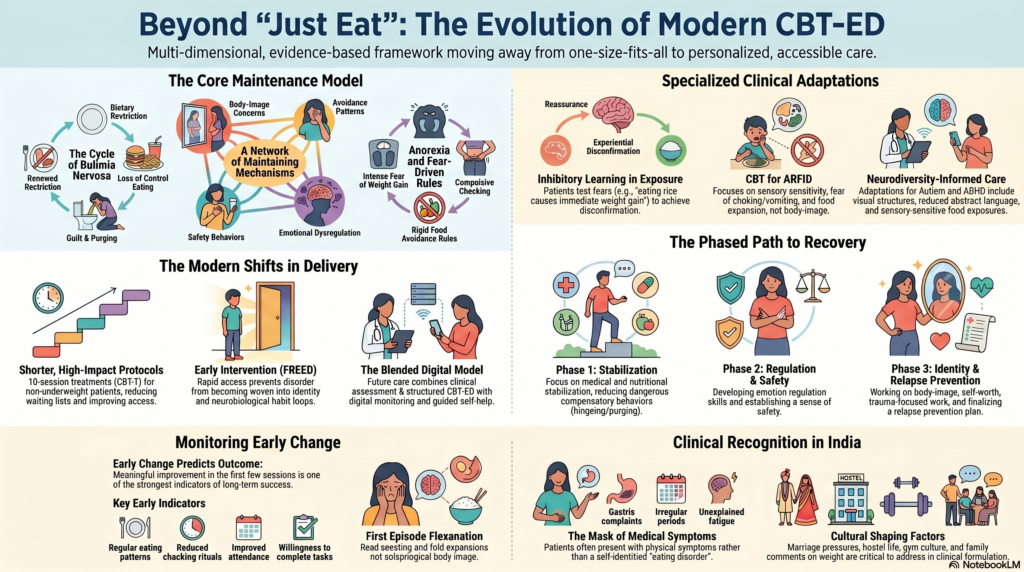
CBT-ED is not one single rigid protocol. It is a family of cognitive-behavioural interventions designed specifically for eating disorder psychopathology. Its central assumption is that disturbed eating behaviour is maintained by a network of thoughts, emotions, behaviours, body-image concerns, avoidance patterns, and safety behaviours.
For example, a patient with bulimia nervosa may enter a cycle of dietary restriction, loss of control eating, guilt, purging, and renewed restriction. A patient with anorexia nervosa may experience intense fear of weight gain, body-image distortion, compulsive checking, rigid food rules, and avoidance of feared foods. A patient with binge-eating disorder may use food as an emotion regulation strategy, followed by shame and self-criticism.
CBT-ED works by identifying these maintaining mechanisms and changing them systematically.
Why CBT-ED Matters
The recent review by Waller and Beard highlights a crucial point: CBT-ED has good evidence, but the field cannot afford complacency. Recovery rates are still imperfect, relapse remains a concern, and outcomes are particularly challenging in anorexia nervosa. The goal is not merely to prove that CBT-ED works; the next step is to improve how quickly, how widely, and how precisely it works.
This is especially relevant in real-world clinical practice, where patients often face long waiting lists, limited specialist services, family distress, medical risk, and high dropout rates.
The Shift Toward Briefer and More Efficient CBT
One of the most important recent developments is the move toward brief CBT-ED protocols. Traditional CBT for eating disorders may involve around 20 sessions or more. However, newer models such as CBT-T, a 10-session cognitive behavioural therapy for non-underweight eating disorders, show encouraging outcomes for bulimia nervosa, binge-eating disorder, and related presentations.
This matters clinically because shorter effective treatments can reduce waiting lists, improve access, and allow more patients to receive care earlier.
A practical implication is clear: not every eating disorder patient requires long-term exploratory therapy at the outset. Many patients benefit from a focused, structured, behavioural, and psychoeducational approach that directly targets eating patterns, bingeing, purging, body checking, avoidance, and distorted beliefs.
Online CBT-ED and Digital Access
The COVID-19 pandemic forced mental health services to rethink delivery. CBT-ED, traditionally delivered face-to-face, has increasingly been offered through telehealth and online formats. The evidence reviewed suggests that online delivery is feasible and may improve accessibility, especially when specialist services are scarce.
However, digital interventions should not be confused with fully validated therapy. Apps, self-help modules, and internet-based interventions can be useful adjuncts, but they should not replace skilled clinical assessment and monitoring, especially in medically risky eating disorders.
The future likely lies in a blended model:
clinical assessment + structured CBT-ED + guided self-help + digital monitoring + relapse prevention.
Early Intervention: Treat Before the Disorder Becomes Entrenched
Another major advance is the focus on early intervention. Programmes such as FREED — First Episode Rapid Early Intervention for Eating Disorders — aim to reduce the duration of untreated eating disorder and provide rapid access to treatment in young people and early-stage illness.
This is an important conceptual shift. In psychiatry, we already recognise early intervention in psychosis and mood disorders. Eating disorders deserve the same urgency.
The longer an eating disorder persists, the more it may become woven into identity, family systems, rituals, social functioning, and neurobiological habit loops. Early CBT-ED may prevent this consolidation.
Yet the review also makes an important corrective point: long duration does not mean treatment is futile. Even patients with longstanding eating disorders can benefit from structured therapy. Duration alone should not be used to deny recovery-oriented treatment.
CBT-ED in Adolescents and Young People
Family-Based Treatment remains a major evidence-based approach for children and adolescents, especially in anorexia nervosa. But CBT-ED is increasingly being recognised as useful for young people in selected situations.
CBT-ED may be considered when family-based treatment is unavailable, unacceptable, partially effective, or when the adolescent needs a more individualised cognitive-behavioural formulation.
This is particularly relevant in older adolescents and transition-age youth, where autonomy, identity, peer comparison, social media exposure, body image, perfectionism, and emotional regulation all play important roles.
Exposure Therapy and Inhibitory Learning
A modern CBT-ED approach is not just about “talking differently about food.” It involves behavioural change.
One important development is the use of exposure therapy based on inhibitory learning. In eating disorders, feared foods, fullness, weight gain, body sensations, and social eating can all become anxiety triggers.
Traditional exposure aims to reduce fear through repetition. Inhibitory learning goes further. It helps the patient learn:
“This feared situation is uncomfortable, but it is not dangerous.”
For example, a patient may predict, “If I eat rice, I will lose control and gain weight immediately.” CBT-ED exposure allows the patient to test this prediction, tolerate distress, and build new learning.
The aim is not reassurance. The aim is experiential disconfirmation.
CBT for ARFID
Avoidant/Restrictive Food Intake Disorder, or ARFID, is an important and often under-recognised eating disorder. Unlike anorexia nervosa, ARFID is not primarily driven by fear of fatness or body-image disturbance. It may involve sensory sensitivity, fear of choking or vomiting, low appetite, food neophobia, gastrointestinal concerns, or traumatic food experiences.
CBT-ED adapted for ARFID uses exposure, behavioural experiments, anxiety reduction, sensory work, and gradual food expansion. Recent research suggests this is a promising area, though more definitive evidence is still needed.
This is especially relevant in child psychiatry, neurodevelopmental clinics, gastroenterology-linked cases, and patients mislabelled as “fussy eaters.”
Trauma, Compassion and Treatment Matching
One of the most clinically meaningful developments is the recognition that eating disorders may interact with trauma histories. Trauma does not cause every eating disorder, but in some patients, food, body control, dissociation, shame, disgust, and self-punishment may be linked to earlier adverse experiences.
Recent evidence suggests that some trauma-associated eating disorder presentations may benefit from integrating approaches such as EMDR or compassion-focused therapy alongside CBT-ED.
This does not mean every patient needs trauma processing immediately. In fact, premature trauma work in an unstable patient may worsen symptoms. A phased approach is often wiser:
- Medical and nutritional stabilisation
- Reduction of bingeing, purging, starvation, or compensatory behaviours
- Emotion regulation and safety
- Body-image and self-worth work
- Trauma-focused work where indicated
- Relapse prevention
The key is formulation-based care rather than protocol worship.
Early Change Predicts Outcome
One of the strongest clinical lessons from CBT-ED research is that early change matters. Patients who show meaningful improvement in the first few sessions are more likely to do well later. This has practical value.
Clinicians should monitor early behavioural indicators such as:
regular eating,
reduced purging,
reduced binge episodes,
increased food flexibility,
reduced weighing/checking rituals,
improved session attendance,
willingness to complete between-session tasks.
If there is no early change, therapy should not simply continue mechanically. The clinician must ask:
Is the formulation correct?
Is the patient medically unstable?
Is there hidden purging or laxative use?
Is trauma, autism, ADHD, depression, OCD, or substance use complicating treatment?
Is the family maintaining symptoms unintentionally?
Is the patient afraid of recovery itself?
CBT-ED is structured, but it should never be blind.
Neurodiversity and Eating Disorders
The review also highlights neurodiversity as an important future direction. Autism and ADHD can complicate eating disorder assessment and treatment. Some patients may have sensory sensitivities, rigidity, interoceptive difficulties, impulsivity, emotional dysregulation, or executive dysfunction.
In such cases, standard CBT-ED may need adaptation:
more visual structure,
clearer session agendas,
reduced abstract language,
sensory-sensitive food exposure,
executive function supports,
family involvement where appropriate,
slower pacing,
predictable homework formats.
This is a major frontier for eating disorder care. A patient should not be labelled “resistant” when the therapy format itself has not been adapted to the brain in front of us.
Digital Tools: Promise, But Not Yet a Replacement
Apps and digital interventions are attractive because they are scalable and inexpensive. They can help with food logs, symptom tracking, reminders, psychoeducation, and relapse monitoring.
But the evidence is still not strong enough to claim that apps alone can treat eating disorders safely. This is especially true for anorexia nervosa, severe purging, electrolyte risk, suicidality, or complex comorbidity.
The future should be digital-assisted therapy, not digitally abandoned patients.
The Indian Clinical Context
In India, eating disorders are often underdetected. Many patients present not with the words “eating disorder,” but with:
gastric complaints,
weight loss,
irregular periods,
fatigue,
academic decline,
excessive exercise,
body dissatisfaction,
“dieting,”
vomiting after meals,
family conflict around food,
or repeated consultations for unexplained medical symptoms.
Cultural factors also matter. Thinness, marriage pressures, social media ideals, gym culture, dance/sports demands, hostel life, perfectionism, and family comments about weight can all shape eating pathology.
CBT-ED offers an excellent framework for Indian practice because it is structured, psychoeducational, measurable, and adaptable. It can be integrated into psychiatry OPDs, clinical psychology services, adolescent clinics, gastroenterology referrals, and multidisciplinary care.
Practical Clinical Message
CBT-ED has moved beyond the old idea of simply “correcting distorted thoughts.” Modern CBT-ED is behavioural, emotional, relational, developmental, and increasingly personalised.
The best outcomes are likely when treatment is:
early,
structured,
measurement-based,
medically informed,
family-sensitive,
trauma-aware,
neurodiversity-informed,
and relapse-focused.
Eating disorders do not improve by advice alone. Telling a patient to “just eat” is like telling a person with OCD to “just stop checking.” The symptom has a function. Treatment must understand that function and then help the patient build a safer, freer life.
Conclusion
CBT-ED remains one of the most evidence-supported treatments for eating disorders, but the field is evolving rapidly. Briefer protocols, online delivery, early intervention, ARFID-specific approaches, inhibitory learning, trauma-informed adaptations, neurodiversity-sensitive modifications, and clinician competence measures are shaping the next generation of care.
The future of eating disorder treatment will not be one-size-fits-all. It will be structured but flexible, evidence-based but humane, and protocol-driven but formulation-guided.
Recovery is not simply about normalising food. It is about restoring agency, embodiment, emotional freedom, and dignity.
Dr. Srinivas Rajkumar T, MD (AIIMS,new Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery, Chennai
✉ srinivasaiims@gmail.com 📞 +91-8595155808
Related posts:
- Cognitive Behavioural Therapy (CBT) for Depression – Treatment without medications
- Breaking the Cycle: An Introduction to Cognitive Behavioural Therapy (CBT)
- What Does a Cognitive Behavioral Therapy (CBT) Session Look Like?
- Cognitive-behavioral therapy (CBT) – Terms and Terminologies
- Cognitive Behavioural Therapy for OCD
- When Should Lisdexamfetamine Be Considered for Binge Eating Disorder?