Role of a Psychiatrist in Alcoholism Recovery: From Detoxification to Relapse Prevention
 Alcohol recovery is not simply a matter of “willpower” or “just stopping.” In a person who has developed alcohol dependence, the brain and body have adapted to the regular presence of alcohol. When alcohol is suddenly stopped, the person may develop withdrawal symptoms — tremors, sweating, anxiety, sleeplessness, irritability, high blood pressure, seizures or delirium tremens.
Alcohol recovery is not simply a matter of “willpower” or “just stopping.” In a person who has developed alcohol dependence, the brain and body have adapted to the regular presence of alcohol. When alcohol is suddenly stopped, the person may develop withdrawal symptoms — tremors, sweating, anxiety, sleeplessness, irritability, high blood pressure, seizures or delirium tremens.
This is why the psychiatrist has a central role in alcohol recovery. The psychiatrist helps the patient move safely from alcohol dependence to medically supervised detoxification, then to anti-craving medication, psychological relapse prevention, family support, and finally a long-term recovery plan.
A good alcohol recovery plan does not ask only:
“Can the patient stop drinking?”
It asks:
“Can the patient stop safely, stay stopped, rebuild life, prevent relapse and manage craving without returning to alcohol?”
Alcohol dependence: why stopping suddenly can be dangerous
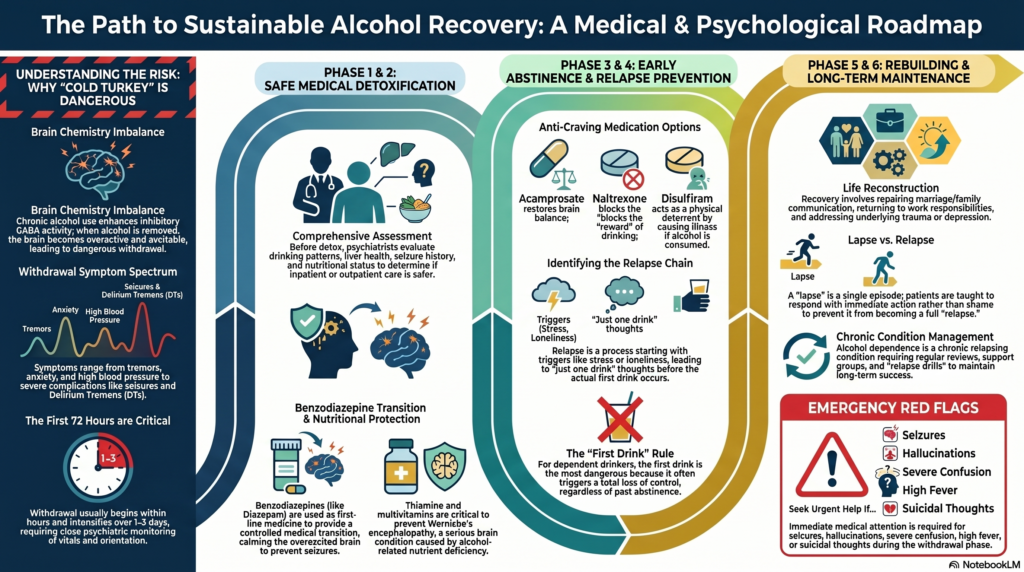
In alcohol dependence, the brain becomes used to alcohol’s calming effect. Alcohol enhances inhibitory GABA activity and affects glutamate systems. Over time, the brain compensates by becoming more excitable. When alcohol is suddenly removed, the brain may become overactive.
This can produce alcohol withdrawal symptoms such as:
tremors, sweating, anxiety, palpitations, nausea, insomnia, irritability, restlessness, high blood pressure, seizures, confusion, hallucinations and delirium tremens.
Benzodiazepines are widely recommended as first-line medicines for alcohol withdrawal, with long-acting agents such as diazepam or chlordiazepoxide commonly preferred; shorter-acting medicines such as lorazepam or oxazepam may be preferred in older adults or liver impairment.
This is the first major role of the psychiatrist: to make stopping alcohol safe.
Step 1: Assessment before detoxification
Before detoxification, the psychiatrist assesses:
quantity and pattern of alcohol use,
duration of drinking,
morning drinking,
previous withdrawal symptoms,
history of withdrawal seizures,
history of delirium tremens,
liver disease,
blood pressure,
diabetes,
gastritis,
pancreatitis,
head injury,
sleep problems,
depression,
anxiety,
suicide risk,
other substance use,
family support,
and motivation for abstinence.
The psychiatrist also decides whether detoxification can be done as an outpatient or whether inpatient admission is safer. Severe dependence, history of seizures, delirium tremens, medical instability, poor support, high suicide risk, pregnancy, severe liver disease or polysubstance use may require inpatient care.
NICE guidance on alcohol-use disorders recommends structured assessment and management of harmful drinking and alcohol dependence, including matching the intensity of treatment to the severity and risks of dependence.
Step 2: Detoxification — the smooth transition from alcohol to safer medication
Alcohol withdrawal treatment is essentially a controlled medical transition.
The person is moving from alcohol, an unsafe and damaging sedative, to a carefully dosed medicine that prevents withdrawal complications. In many cases, this medicine is a benzodiazepine.
This is not “replacing one addiction with another.” In detoxification, benzodiazepines are used short-term, in a planned, tapering manner, to calm the overexcited brain and prevent dangerous withdrawal.
The aim is to prevent:
withdrawal seizures,
severe agitation,
autonomic instability,
hallucinations,
delirium tremens,
sleeplessness,
and early dropout from treatment.
A psychiatrist may use either:
fixed-dose detoxification, where the dose is planned and reduced gradually, or
symptom-triggered detoxification, where medicine is given based on withdrawal severity.
The choice depends on setting, severity, monitoring availability and patient risk.
Step 3: Thiamine and medical protection
Alcohol dependence is often associated with poor nutrition and thiamine deficiency. This can lead to Wernicke’s encephalopathy, a serious brain condition that may cause confusion, eye movement abnormalities, imbalance and later memory problems.
Therefore, detoxification is not only benzodiazepines. A proper plan often includes:
thiamine,
multivitamins,
hydration,
sleep correction,
nutrition,
liver function assessment,
blood tests,
management of gastritis,
blood pressure monitoring,
diabetes monitoring,
and screening for depression or suicidality.
In people with alcohol dependence, thiamine is often given before glucose-containing fluids when deficiency is suspected, because glucose can precipitate or worsen Wernicke’s encephalopathy in vulnerable patients.
Step 4: The first week — stabilising the body and mind
The first few days are often the most medically important. Withdrawal usually begins within hours after the last drink and can intensify over the next 1–3 days. Some patients develop delayed complications, especially if there is severe dependence.
During this phase, the psychiatrist monitors:
tremors, sweating, pulse, blood pressure, sleep, anxiety, confusion, hallucinations, orientation, hydration, seizure risk and medication response.
The goal is not to sedate the patient heavily. The goal is to keep the patient calm, oriented, medically safe and able to continue treatment.
This is also the phase where many patients say:
“Doctor, I feel better now. I think I can drink occasionally.”
That is a high-risk thought. Detoxification only clears the withdrawal phase. It does not cure dependence. The next phase is relapse prevention.
Step 5: After detoxification — why anti-craving medication matters
Once withdrawal settles, the brain is still vulnerable. Craving, sleep disturbance, emotional discomfort, social triggers and habit memory can pull the person back to alcohol.
This is where anti-craving and relapse-prevention medications become important.
Commonly used medicines include:
acamprosate,
naltrexone,
disulfiram,
and selected off-label medicines in specific cases.
The choice depends on the patient’s goal, liver function, kidney function, craving type, impulsivity, family supervision, medical history and treatment preference.
The American Psychiatric Association guideline supports pharmacotherapy, usually along with psychosocial interventions, for patients with moderate to severe alcohol use disorder.
Acamprosate: how it helps prevent craving
Acamprosate is especially useful for maintaining abstinence after detoxification. It is commonly used when the goal is complete abstinence rather than controlled drinking.
Many patients ask, “Does acamprosate work like alcohol?”
A simple explanation is this:
Acamprosate is not alcohol, and it does not produce intoxication. But it helps calm the alcohol-adapted brain by restoring balance in the brain’s glutamate-GABA systems.
Alcohol repeatedly pushes the brain in one direction. After stopping alcohol, the brain remains restless, overexcitable and craving-prone. Acamprosate helps reduce this biological restlessness. In that limited sense, patients sometimes understand it as a “substitute signal” that helps the brain stay steady without alcohol — but medically, it is better described as a glutamate-modulating anti-craving medicine, not as “artificial alcohol.”
It can help reduce:
background craving,
inner restlessness,
emotional discomfort after stopping alcohol,
risk of relapse,
and the feeling that “something is missing.”
Acamprosate works best when the person has already stopped drinking and is motivated for abstinence. It is usually not a medicine for acute withdrawal. It is a maintenance medicine for relapse prevention.
Naltrexone: reducing the reward from alcohol
Naltrexone works differently. It blocks opioid receptors involved in the rewarding effect of alcohol. It may reduce the “high,” pleasure, reinforcement and heavy-drinking relapse risk.
It may be useful for patients who say:
“Once I start, I cannot stop.”
“I drink for the kick.”
“I relapse during social drinking.”
“One peg becomes one bottle.”
Naltrexone requires liver function consideration and is not used in patients taking opioids.
Disulfiram: creating a deterrent
Disulfiram works by producing an unpleasant reaction if alcohol is consumed. It can cause flushing, nausea, vomiting, palpitations, headache and distress after drinking alcohol.
It is not an anti-craving medicine in the same way as acamprosate or naltrexone. It is a deterrent. It works best when the patient is highly motivated and family supervision is available.
It should not be used casually or secretly. The patient must understand the reaction and give informed consent.
Step 6: Psychological interventions — the real foundation of long-term recovery
Medicines reduce withdrawal and craving. But long-term recovery requires psychological work.
Alcohol is rarely only a chemical. It often becomes linked to:
stress relief,
loneliness,
sleep,
celebration,
anger,
boredom,
social identity,
masculinity,
work pressure,
trauma,
marital conflict,
financial stress,
or avoidance of emotional pain.
If these links are not addressed, relapse risk remains high.
Psychological interventions for alcohol use disorder commonly include motivational enhancement, cognitive behavioural therapy, relapse prevention, behavioural self-control, family interventions, and mutual-help or recovery-support approaches.
Relapse prevention: identifying the high-risk chain
Relapse does not usually happen suddenly. It follows a chain.
A common relapse chain looks like this:
stress → poor sleep → irritability → craving → “just one drink” thought → meeting old drinking friend → first drink → loss of control → guilt → continued drinking.
The psychiatrist helps the patient identify this chain early.
Important relapse triggers include:
salary day,
weekends,
loneliness,
marital conflict,
work stress,
old drinking friends,
parties,
bars,
travel,
pain,
insomnia,
sexual frustration,
anger,
shame,
boredom,
and overconfidence after a few weeks of abstinence.
The goal is to catch relapse before the first drink.
The “first drink” rule
For a dependent drinker, the first drink is often the most dangerous drink.
Many patients do not relapse because they planned to drink heavily. They relapse because they believed they could drink moderately.
Common relapse thoughts include:
“I am cured now.”
“I will drink only beer.”
“I will drink only on weekends.”
“I will not drink alone.”
“I will stop after two pegs.”
“I deserve it after so much stress.”
“This is a special occasion.”
“I can control it now.”
Relapse prevention teaches the patient to treat these thoughts as warning signs, not decisions.
Urge surfing and craving management
Craving usually rises, peaks and falls like a wave. It feels permanent in the moment, but it often reduces if the person does not act on it.
Techniques include:
delaying the decision by 20–30 minutes,
drinking water or eating something,
leaving the trigger situation,
calling a support person,
walking,
cold shower,
breathing exercise,
writing the craving score,
remembering past consequences,
and using prescribed anti-craving medication regularly.
The patient is taught:
Craving is a signal, not a command.
Managing sleep without alcohol
Many alcohol-dependent patients use alcohol as a sleep medicine. After stopping, sleep may initially worsen. This becomes a major relapse trigger.
A psychiatrist helps by treating insomnia safely through:
sleep hygiene,
fixed wake time,
avoiding daytime naps,
reducing caffeine,
relaxation training,
treating anxiety or depression,
short-term medication if needed,
and avoiding long-term sedative dependence.
This is crucial because poor sleep often brings back craving.
Treating depression and anxiety
Many patients drink because they are depressed or anxious. Others become depressed and anxious because of alcohol. Often both are true.
A psychiatrist assesses:
primary depression,
alcohol-induced depression,
anxiety disorder,
panic symptoms,
trauma,
suicidal thoughts,
bipolar disorder,
ADHD,
personality vulnerabilities,
and sleep disorders.
This matters because untreated depression or anxiety can sabotage recovery. At the same time, symptoms may improve significantly after sustained abstinence, so timing and follow-up are important.
Family involvement: support without policing
Alcohol dependence affects the entire family. Spouses, parents and children often live with fear, anger, disappointment and mistrust.
Family work includes:
explaining dependence as a treatable disorder,
reducing blame,
setting boundaries,
creating a safe home environment,
removing alcohol access,
monitoring medication where appropriate,
planning for salary days and social functions,
identifying relapse warning signs,
and avoiding both overcontrol and enabling.
Family members should not become jailers. But they can become recovery allies.
The comprehensive alcohol recovery plan
A good recovery plan usually has several phases.
Phase 1: Engagement and motivation
The psychiatrist helps the patient understand:
what alcohol has done to health, family, work and dignity,
what triggers drinking,
what previous quit attempts show,
why withdrawal must be managed safely,
and what recovery can realistically look like.
Motivation is strengthened, not forced.
Phase 2: Medical detoxification
This phase includes:
withdrawal-risk assessment,
benzodiazepine-based detoxification when indicated,
thiamine and nutritional support,
medical monitoring,
sleep management,
seizure prevention,
delirium monitoring,
and family education.
The goal is safe alcohol cessation.
Phase 3: Early abstinence
This is the first few weeks after detox. The patient may feel physically better but psychologically vulnerable.
Treatment includes:
anti-craving medication,
sleep stabilisation,
daily routine,
avoiding high-risk people and places,
frequent follow-up,
family supervision,
and management of anxiety, depression or irritability.
This phase is high risk because overconfidence begins early.
Phase 4: Relapse prevention
This phase focuses on:
trigger mapping,
craving management,
refusal skills,
stress management,
anger management,
financial planning,
weekend planning,
social restructuring,
exercise,
meaningful activity,
and emergency relapse plan.
The patient learns not only how to stop drinking, but how to live without alcohol.
Phase 5: Repair and rebuilding
Once abstinence stabilises, deeper work begins:
rebuilding trust,
improving marriage and family communication,
returning to work responsibility,
managing shame and guilt,
addressing trauma,
treating comorbid psychiatric problems,
repairing finances,
building self-respect,
and creating a new identity beyond alcohol.
This is where recovery becomes more than abstinence. It becomes reconstruction.
Phase 6: Long-term maintenance
Alcohol dependence is a chronic relapsing condition, but relapse is not inevitable. Long-term maintenance includes:
regular review,
continuing anti-craving medication when useful,
monitoring liver and metabolic health,
psychotherapy follow-up,
support group participation if acceptable,
family review,
relapse drills,
and early intervention if lapses occur.
The patient should know exactly what to do if craving returns or if a lapse happens.
Lapse versus relapse
A lapse is a single episode or brief return to drinking. A relapse is a return to the old pattern.
The psychiatrist teaches the patient and family not to respond to a lapse with shame and hopelessness.
The right response is:
stop immediately,
inform the treating doctor or support person,
analyse the trigger,
restart the plan,
adjust medication if needed,
increase follow-up,
and prevent the lapse from becoming a relapse.
One drink does not have to become one month of drinking.
What makes a recovery plan successful?
A good plan is:
medical,
psychological,
family-based,
structured,
realistic,
non-judgemental,
and long-term.
It includes:
safe detoxification,
benzodiazepine transition where required,
thiamine and medical care,
anti-craving medication such as acamprosate or naltrexone,
psychological relapse prevention,
family involvement,
sleep and mood treatment,
lifestyle restructuring,
and regular follow-up.
The best outcomes happen when treatment does not stop after detoxification.
Detoxification is only the doorway. Recovery is the path after that.
When should someone seek urgent help?
Immediate medical help is needed if a person stopping alcohol develops:
seizures,
confusion,
hallucinations,
severe tremors,
high fever,
severe agitation,
very high blood pressure,
disorientation,
repeated vomiting,
head injury,
suicidal thoughts,
or inability to eat or drink.
Alcohol withdrawal can be life-threatening. It should not be underestimated.
Conclusion
The psychiatrist’s role in alcoholism recovery is central because alcohol dependence affects the brain, body, behaviour, family and future.
The first job is safety: detoxification, withdrawal control, seizure prevention and smooth transition from alcohol to medically supervised treatment.
The second job is stability: anti-craving medicines such as acamprosate, sleep correction, mood treatment and early abstinence support.
The third job is recovery: psychological relapse prevention, family involvement, lifestyle restructuring and long-term follow-up.
A comprehensive alcohol recovery plan does not shame the patient. It gives the patient a map.
Stop safely.
Prevent craving.
Understand triggers.
Build skills.
Repair life.
Stay connected.
Restart quickly if there is a lapse.
That is how recovery becomes sustainable.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808