Alcohol Detoxification on OPD Basis
 Quitting Alcohol Without Admission: When It Is Possible, When It Is Unsafe
Quitting Alcohol Without Admission: When It Is Possible, When It Is Unsafe
Alcohol detoxification means safely managing withdrawal symptoms after stopping or reducing alcohol. Many people assume that quitting alcohol always requires hospital admission. That is not always true.
For selected patients, alcohol detoxification can be done on an OPD/outpatient basis with medicines, family supervision, daily monitoring, and a clear emergency plan. But it must be done carefully because alcohol withdrawal can sometimes become dangerous.
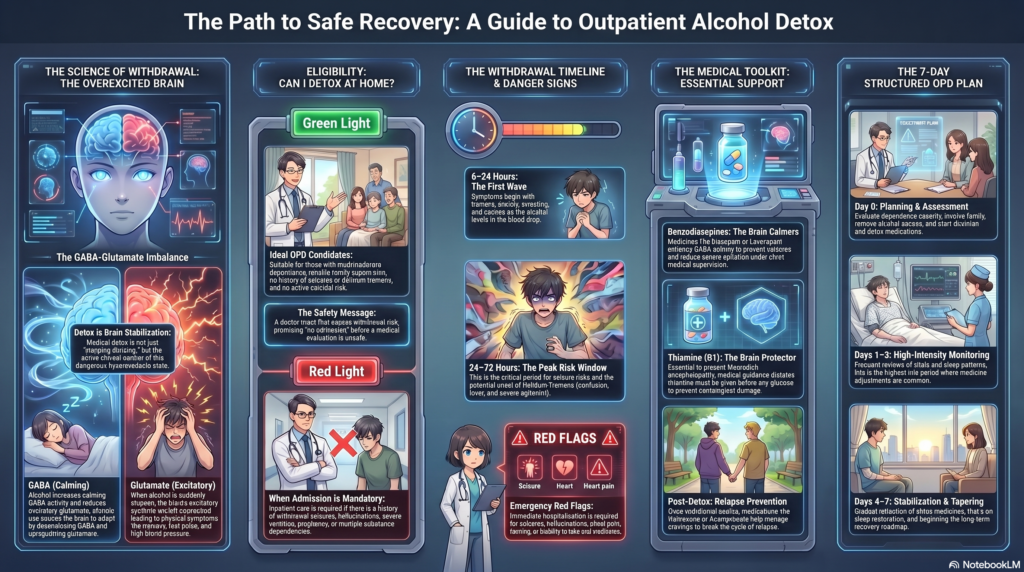
Alcohol withdrawal may begin within 6–24 hours after reduction or cessation of heavy drinking and can include tremors, insomnia, nausea, anxiety, agitation, hallucinations, seizures, and delirium tremens if severe or undertreated.
Why Alcohol Withdrawal Happens
Alcohol acts mainly by increasing inhibitory GABA activity and reducing excitatory glutamate activity in the brain.
With repeated heavy drinking, the brain adapts:
- GABA calming systems become less sensitive.
- Glutamate excitatory systems become upregulated.
- Stress chemicals increase.
- Sleep and autonomic regulation become disturbed.
When alcohol is suddenly stopped, the brain is left in an overexcited state.
This produces:
- shaking
- sweating
- anxiety
- fast pulse
- high BP
- insomnia
- irritability
- nausea
- craving
- hallucinations
- seizures in severe cases
So alcohol detox is not just “stopping drinking.” It is controlling a hyperexcitable brain state.
Can Alcohol Detox Be Done on OPD Basis?
Yes, OPD alcohol detoxification is possible in carefully selected patients.
It is usually suitable when:
- dependence is mild to moderate
- there is no history of withdrawal seizures
- no history of delirium tremens
- no severe liver disease or medical instability
- no active suicidal risk
- no severe psychiatric instability
- patient has reliable family support
- patient can attend frequent follow-up
- patient can take medicines responsibly
- there is no ongoing heavy intoxication
- there is safe home monitoring
AAFP guidance notes that patients with mild to moderate withdrawal symptoms without major risk factors can often be treated in outpatient settings, while those with severe or complicated symptoms need inpatient care.
Who Should NOT Do OPD Detox?
Some patients should not attempt home detox.
Admission is safer if there is:
- past withdrawal seizure
- past delirium tremens
- confusion or disorientation
- hallucinations
- severe tremors
- severe vomiting
- dehydration
- very high pulse or BP
- uncontrolled diabetes, hypertension, heart disease, liver disease, pancreatitis, or infection
- pregnancy
- elderly frailty
- multiple substance use
- benzodiazepine dependence
- suicidal thoughts
- psychosis or severe mood disorder
- no reliable family member at home
- repeated failed home detox attempts
- very heavy daily drinking
- poor ability to follow instructions
Delirium tremens is a medical emergency, typically occurring around 48–72 hours after the last drink, with confusion, agitation, autonomic instability, and risk of seizures. It requires urgent hospital-level treatment.
What Happens in OPD Alcohol Detox?
OPD detox is not casual advice. It is a structured medical plan.
Step 1: Assessment
The doctor assesses:
- amount of alcohol used daily
- duration of drinking
- time of last drink
- morning drinking
- withdrawal symptoms
- previous seizures or DT
- medical illness
- liver function
- psychiatric history
- sleep
- nutrition
- motivation
- family support
- suicide risk
- use of other substances
- current medicines
Basic tests may include:
- CBC
- liver function test
- renal function
- electrolytes
- blood sugar
- ECG if indicated
- GGT, MCV, ultrasound, viral markers if clinically needed
Step 2: Withdrawal Risk Stratification
Patients are usually divided into:
Low risk
- mild tremor
- mild anxiety
- mild insomnia
- no seizure history
- stable vitals
- good family support
May be managed with OPD medicines and close monitoring.
Moderate risk
- clear withdrawal symptoms
- significant craving
- autonomic symptoms
- moderate dependence
- but no seizures, no confusion, no severe medical instability
May still be managed on OPD basis by an experienced clinician, with closer follow-up.
High risk
- seizures
- confusion
- hallucinations
- severe autonomic instability
- serious medical illness
- unreliable supervision
Needs admission.
Medicines Used in Alcohol Detox
1. Benzodiazepines
Benzodiazepines are the main medicines used to prevent severe withdrawal, seizures, and delirium.
Common options include:
- diazepam
- chlordiazepoxide
- lorazepam
- oxazepam
Long-acting benzodiazepines such as chlordiazepoxide or diazepam are commonly recommended for alcohol withdrawal symptom control.
Why benzodiazepines help
They calm the overexcited brain by enhancing GABA activity.
They reduce:
- tremors
- anxiety
- insomnia
- agitation
- seizure risk
- progression to severe withdrawal
Important caution
These medicines should be used only under medical supervision because they can cause:
- sedation
- falls
- respiratory depression
- misuse
- worsening confusion
- interaction with alcohol
They should not be mixed with alcohol.
2. Thiamine
Thiamine, or vitamin B1, is essential in alcohol detox.
Alcohol dependence commonly causes thiamine deficiency, which can lead to Wernicke’s encephalopathy, a serious neurological emergency.
Indian standard treatment guidance for alcohol dependence recommends thiamine supplementation during withdrawal management and warns that glucose should not be given without thiamine in withdrawal care.
Why thiamine is important
It helps prevent:
- confusion
- memory problems
- ataxia
- Wernicke-Korsakoff syndrome
In higher-risk patients, injectable thiamine may be needed.
3. Vitamins and Nutrition
Patients may need:
- multivitamins
- folate
- B-complex
- magnesium correction if deficient
- hydration
- protein-rich diet
- sleep restoration
Alcohol dependence is often associated with nutritional depletion.
4. Anti-craving Medicines After Detox
Detox is only the first step.
After withdrawal settles, relapse prevention medicines may be considered.
Options include:
- naltrexone
- acamprosate
- disulfiram
- baclofen in selected cases
- topiramate in selected cases
Choice depends on:
- liver function
- kidney function
- craving pattern
- drinking goal
- psychiatric comorbidity
- family supervision
- adherence
- patient preference
OPD Detox: What the Family Must Monitor
Family supervision is extremely important.
Monitor:
- pulse
- BP if possible
- sleep
- tremors
- sweating
- confusion
- irritability
- hallucinations
- vomiting
- fluid intake
- food intake
- medicine adherence
- alcohol access
- suicidal thoughts
- unusual behaviour
The patient should not drive, work with machinery, make major decisions, or be left alone during the high-risk withdrawal period.
Red Flag Symptoms: Go to Hospital Immediately
Emergency care is needed if there is:
- seizure
- confusion
- disorientation
- hallucinations
- severe agitation
- severe vomiting
- dehydration
- fever
- chest pain
- breathlessness
- severe drowsiness
- fainting
- uncontrolled BP or pulse
- suicidal behaviour
- repeated drinking during detox
- inability to take oral medicines
- worsening tremors despite medicines
Do not wait at home if these occur.
Typical Timeline of Alcohol Withdrawal
6–12 hours
- tremor
- anxiety
- sweating
- nausea
- craving
- insomnia
12–24 hours
- worsening tremor
- irritability
- raised pulse
- raised BP
- restlessness
24–48 hours
- seizure risk period
- hallucinations may appear
- autonomic symptoms may worsen
48–72 hours
- risk of delirium tremens in vulnerable patients
- confusion, agitation, fever, severe autonomic instability
3–7 days
- symptoms gradually improve in uncomplicated withdrawal
Weeks later
Some patients have prolonged symptoms:
- sleep disturbance
- low mood
- irritability
- craving
- poor concentration
- anxiety
This is called protracted withdrawal or post-acute withdrawal.
Common Patient Fear: “Will I Need Admission?”
Not everyone needs admission.
Admission is mainly needed when withdrawal is likely to be medically risky. Many patients with mild to moderate alcohol dependence can quit with OPD-based detox if properly assessed and monitored.
But it is unsafe to promise “no admission” before assessment.
A safer message is:
“We will first assess your withdrawal risk. If it is mild to moderate and you have good home support, OPD detox may be possible. If there are danger signs, admission is safer.”
What OPD Detox Is NOT
OPD detox is not:
- suddenly stopping alcohol without medicines
- taking sleeping pills randomly
- self-medicating with benzodiazepines
- drinking “small amounts” whenever withdrawal starts
- relying only on willpower
- hiding symptoms from family
- skipping follow-up
- detoxing alone in a room
Alcohol withdrawal can be dangerous. Medical supervision matters.
Practical OPD Detox Plan
A structured OPD plan usually includes:
Day 0: Assessment and planning
- evaluate dependence severity
- check vitals
- assess withdrawal risk
- involve family member
- prescribe detox medicines
- start thiamine
- remove alcohol access
- plan follow-up
Day 1–3: Highest monitoring period
- frequent review
- monitor sleep, tremor, pulse, BP
- adjust medicines if needed
- watch for red flags
- ensure hydration and nutrition
Day 4–7: Stabilization
- taper detox medicines
- manage sleep
- address craving
- begin relapse prevention planning
Week 2 onwards: Recovery phase
- anti-craving medication if needed
- counselling
- family work
- routine building
- treatment of depression, anxiety, ADHD, trauma, or insomnia if present
- relapse prevention
Why Detox Alone Is Not Enough
Detox removes alcohol from the body.
But treatment must also address:
- craving
- stress
- habit
- sleep
- emotional triggers
- social pressure
- relationship conflict
- psychiatric comorbidity
- relapse prevention
- lifestyle structure
Without relapse prevention, detox becomes a repeated cycle:
Stop → withdrawal → restart → guilt → stop again → relapse
The goal is not just abstinence for a few days.
The goal is stable recovery.
Outpatient Detox: Best Candidates
OPD detox works best when the patient says:
- “I am motivated.”
- “I can come for follow-up.”
- “My family can supervise.”
- “I will not hide drinking.”
- “I will avoid driving.”
- “I will take medicines as prescribed.”
- “I will go to hospital if red flags appear.”
- “I am ready for relapse prevention after detox.”
Simple Patient-Friendly Explanation
“Alcohol withdrawal happens because the brain has adjusted to alcohol. When alcohol is suddenly stopped, the brain becomes overexcited. This can cause tremors, anxiety, sweating, sleeplessness, and sometimes seizures or confusion. If your risk is low or moderate, we may be able to manage this safely on OPD basis with medicines, vitamins, family supervision, and daily monitoring. If warning signs appear, hospital admission is safer.”
Key Takeaway
Alcohol detoxification can often be done without admission in selected patients, but it should never be casual or unsupervised.
The safest approach is:
- assess withdrawal risk
- decide OPD vs admission
- use proper medicines
- give thiamine
- involve family
- monitor daily
- treat craving after detox
- build relapse prevention
Quitting alcohol is possible. But the first few days must be handled with respect, planning, and medical supervision.
Need Help to Quit Alcohol Safely?
Alcohol dependence is treatable. Many patients can begin recovery through structured OPD-based detoxification, counselling, anti-craving medication, and relapse prevention planning. The right setting—OPD or admission—depends on withdrawal risk and safety assessment.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808