Bipolar Disorder, Borderline Personality Disorder and ADHD: Why the Differential Diagnosis Matters
 Bipolar disorder, borderline personality disorder and ADHD can look deceptively similar in clinical practice. All three may present with mood swings, irritability, impulsivity, sleep disturbance, racing thoughts, poor frustration tolerance and relationship difficulties. Yet the underlying mechanisms are different, and so is the treatment.
Bipolar disorder, borderline personality disorder and ADHD can look deceptively similar in clinical practice. All three may present with mood swings, irritability, impulsivity, sleep disturbance, racing thoughts, poor frustration tolerance and relationship difficulties. Yet the underlying mechanisms are different, and so is the treatment.
The most useful clinical distinction is this:
Bipolar disorder is primarily episodic mood activation.
Borderline personality disorder is primarily emotional and interpersonal instability.
ADHD is primarily lifelong executive dysfunction with emotional dysregulation.
Misdiagnosis can lead to harm. A person with bipolar disorder may be treated only with antidepressants or stimulants and become more unstable. A person with ADHD may be repeatedly labelled “bipolar” because of restlessness, irritability or impulsivity. A person with borderline personality disorder may receive multiple medications when structured psychotherapy, crisis planning and relational stability are more central.
NICE recommends that suspected bipolar disorder should be assessed with a detailed history of mood episodes, overactivity, disinhibition, symptoms between episodes, triggers, relapse patterns, family history, comorbidities and corroborative information where possible. It also specifically reminds clinicians to consider differential diagnoses such as personality disorders, ADHD, substance use and thyroid disorders.
1. The key clinical question: episode, pattern or trait?
When a patient says, “My mood changes a lot,” the next question should not be, “Is this bipolar?” The better question is:
What is the time course of the change?
In bipolar disorder, the mood change is usually an episode: a clear departure from baseline lasting days to weeks, with changes in energy, sleep, activity, speech, thought speed, confidence, risk-taking and functioning. NICE advises that when adults present with depression, clinicians should ask about previous periods of overactivity or disinhibited behaviour lasting 4 days or more, and consider specialist assessment when present.
In borderline personality disorder, mood shifts are often rapid, reactive and interpersonal. The person may move from confidence to despair, closeness to rejection, anger to guilt, or intense attachment to withdrawal within minutes to hours. NICE describes BPD as involving instability of interpersonal relationships, self-image and mood, impulsive behaviour, fear of abandonment and rejection, and a tendency toward suicidal thinking and self-harm.
In ADHD, the emotional changes are often chronic and situational. The person may become irritable, overwhelmed, restless or dysregulated when bored, delayed, criticised, overstimulated, under-stimulated or required to sustain effort. The core pattern usually begins in childhood and persists across life. NICE states that adult ADHD assessment should consider symptoms that began during childhood, persisted through life, are not better explained by another psychiatric diagnosis, and cause moderate or severe impairment.
2. Bipolar disorder: mood activation, not just mood fluctuation
The defining feature of bipolar disorder is not “mood swings” in a casual sense. It is mood activation.
Activation means that mood, energy, cognition, psychomotor activity and behaviour shift together. The person may sleep less but feel energetic, talk more, think faster, take on multiple plans, spend excessively, become sexually disinhibited, drive recklessly, feel unusually confident or grandiose, become unusually irritable, or show impaired judgement.
A depressive episode in bipolar disorder may look like unipolar depression, but the history may reveal past hypomania, antidepressant-induced activation, family history of bipolar disorder, postpartum mood episodes, psychotic symptoms, mixed features, or recurrent depression with early onset.
Clues favouring bipolar disorder
The following features should raise suspicion:
Mood changes last days to weeks, not minutes to hours.
There is a clear change from baseline.
There is increased energy or goal-directed activity.
Sleep need decreases, but the person does not feel tired.
Impulsivity is limited to activated mood states.
Racing thoughts are accompanied by overconfidence, pressure of speech or increased activity.
There may be grandiosity, expansive mood or marked irritability.
There may be episodic impairment: financial, sexual, occupational, legal, relational or safety-related.
There may be family history of bipolar disorder.
In bipolar disorder, irritability can be severe, but it is usually part of a broader activated syndrome. The patient is not merely angry; they are driven, sleepless, accelerated, disinhibited or unusually energised.
3. Borderline personality disorder: emotional pain, abandonment fear and relational instability
Borderline personality disorder is often misunderstood as “manipulation” or “attention-seeking”. That is both clinically inaccurate and unhelpful. It is better understood as a pattern of intense emotional sensitivity, unstable self-experience, interpersonal threat perception, abandonment fear and impulsive coping.
NIMH describes BPD as involving intense mood swings, uncertainty about self-image, rapidly changing values and feelings, and unstable relationships that may swing between closeness and dislike. It also notes that impulsive behaviours may occur in BPD, but if they occur mainly during elevated mood or energy, a mood disorder should be considered instead.
Clues favouring borderline personality disorder
The following features are clinically useful:
Mood shifts are usually rapid and reactive.
Triggers are often interpersonal: rejection, perceived abandonment, criticism, silence, delay in response, emotional distance or relational ambiguity.
The emotional tone is often anger, shame, emptiness, panic, despair or self-loathing.
There may be chronic feelings of emptiness.
Relationships may be intense and unstable.
There may be recurrent self-harm, suicidal threats or crisis presentations.
Identity may feel unstable: “I don’t know who I am,” “I change depending on who I am with.”
Impulsivity may be self-damaging: spending, substance use, binge eating, unsafe sex, self-injury or sudden relationship decisions.
Transient stress-related paranoid ideation or dissociation may occur.
The key difference from bipolar disorder is that the person usually does not have sustained episodes of increased energy, decreased need for sleep and goal-directed activation. The mood is labile, but not necessarily activated.
4. ADHD: lifelong executive dysfunction with emotional dysregulation
ADHD is not merely distractibility. In adults, it often presents as a disorder of attention regulation, impulse control, time management, emotional regulation, motivation and task initiation.
Many adults with ADHD say:
“I know what to do, but I cannot start.”
“I work only under pressure.”
“My mind keeps jumping.”
“I interrupt without meaning to.”
“I lose things constantly.”
“I am either hyperfocused or completely unable to focus.”
“I get angry quickly, but I cool down quickly.”
“I have always been like this.”
NICE states that ADHD diagnosis should be made by an appropriately qualified specialist using a full clinical and psychosocial assessment, developmental and psychiatric history, observer reports and mental state assessment. It also cautions that ADHD should not be diagnosed solely on the basis of rating scales or observational data.
Clues favouring ADHD
Symptoms begin in childhood, even if not diagnosed then.
Problems are consistent across years, though severity changes with demands.
Inattention, disorganisation, forgetfulness and procrastination are central.
Impulsivity is chronic, not restricted to mood episodes.
Hyperactivity may become inner restlessness in adults.
Mood changes are often short-lived and situational.
Sleep problems may be due to delayed sleep phase, racing mind, poor routine or stimulant/caffeine use.
Emotional dysregulation often follows frustration, boredom, waiting, criticism or overstimulation.
The person may have long-standing academic, occupational or relationship impairment due to inconsistency.
ADHD can mimic hypomania because both may show talkativeness, restlessness, distractibility and impulsivity. The distinction lies in the baseline. In ADHD, these are long-standing traits. In bipolar disorder, they emerge as a noticeable episode.
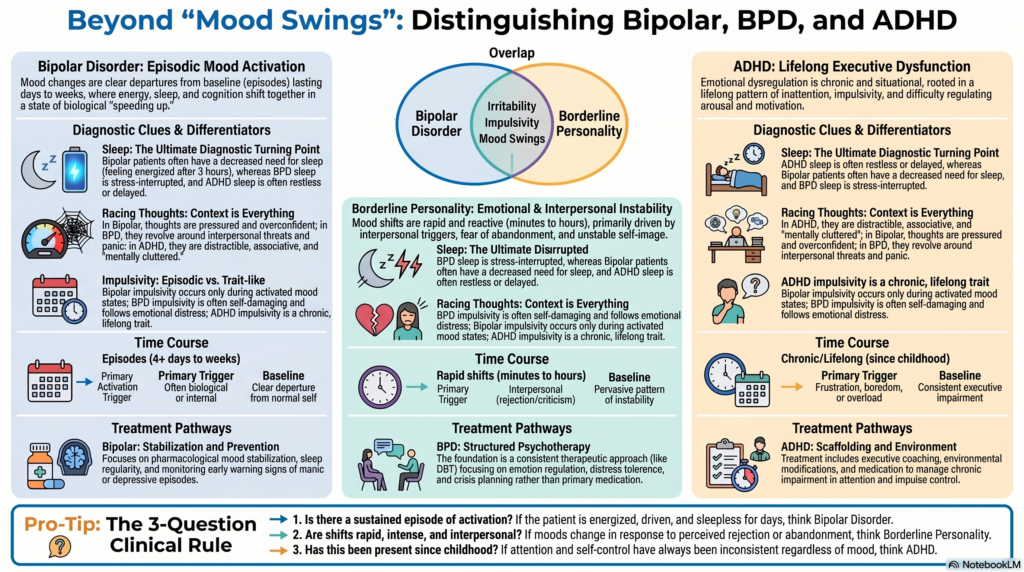
5. Activation versus lability: the most practical distinction
The table in the image captures the most important idea: activation versus lability.
In bipolar disorder, mood change is usually part of a biological activation state. The person does not only feel different; their whole system speeds up or shifts. Sleep, energy, speech, activity, confidence and risk-taking change together.
In borderline personality disorder, mood change reflects affective lability. The person may feel emotionally overwhelmed, abandoned, rejected, empty, furious or terrified. These shifts are often rapid and context-linked.
In ADHD, mood change is usually frustration-based or stimulation-based. The person may become irritable because of delay, boredom, task difficulty, sensory overload, emotional rejection, executive overload or repeated failure.
A simple clinical formulation:
Bipolar disorder: “My mood and energy change in episodes.”
BPD: “My emotions change intensely in relationships and crises.”
ADHD: “My attention, motivation and self-control have always been inconsistent.”
6. Sleep: one of the most useful diagnostic clues
Sleep is often the turning point in diagnosis.
In bipolar hypomania or mania, the patient may sleep very little and still feel energetic. This is not ordinary insomnia. It is decreased need for sleep. The person may sleep 3 hours, wake up refreshed, start projects, message people, spend money or become unusually productive.
In borderline personality disorder, sleep disturbance is often stress-related. Nightmares, trauma reminders, fear of abandonment, interpersonal conflict and emotional arousal may disturb sleep. Poor sleep then worsens impulsivity and emotional regulation.
In ADHD, sleep difficulty is often linked to poor routine, delayed sleep phase, mental restlessness, screen use, procrastination, irregular work cycles or comorbid anxiety. Sleep deprivation worsens ADHD symptoms, but it does not usually produce the expansive, energised syndrome of hypomania.
The question should therefore be:
“When you sleep less, are you tired and worse the next day, or energised and more driven?”
Tired and dysregulated suggests ADHD, anxiety, trauma or BPD. Energised and activated suggests bipolarity.
7. Racing thoughts: same words, different meanings
Patients with all three conditions may report “racing thoughts”.
In bipolar disorder, racing thoughts often come with pressure of speech, increased plans, increased confidence, decreased sleep and accelerated activity.
In borderline personality disorder, racing thoughts may occur during abandonment panic, anger, shame, jealousy, rejection sensitivity or crisis states. The thoughts often revolve around interpersonal threat: “They will leave me,” “I am worthless,” “They don’t care,” “I must do something now.”
In ADHD, racing thoughts are often distractible, associative and task-unrelated. The person may jump from one idea to another, struggle to prioritise, or feel mentally cluttered. There may be novelty-seeking rather than grandiosity.
So, the phrase “racing thoughts” is diagnostically weak unless linked to context, duration, sleep and behaviour.
8. Impulsivity: episodic, self-destructive or executive?
Impulsivity also needs careful parsing.
In bipolar disorder, impulsivity is often episodic. Spending, sexual risk, reckless driving, substance use or grand business plans occur during hypomania or mania and reduce when mood stabilises.
In borderline personality disorder, impulsivity is often emotionally driven and self-damaging. It may follow rejection, emptiness, rage, dissociation or intense distress.
In ADHD, impulsivity is trait-like. The person interrupts, acts before thinking, makes quick decisions, struggles to wait, starts tasks without finishing, blurts out responses, or seeks stimulation. It is not confined to mood episodes.
This distinction is crucial because the treatment target differs. Bipolar impulsivity needs mood stabilisation. BPD impulsivity needs emotion regulation and crisis skills. ADHD impulsivity needs executive scaffolding, environmental modification and ADHD-focused treatment.
9. Can these conditions coexist?
Yes. This is where clinical work becomes more nuanced.
A patient can have ADHD and bipolar disorder. In such cases, the ADHD symptoms are lifelong, but bipolar episodes appear as distinct periods of mood activation. Treatment usually requires stabilising bipolar disorder first before carefully treating ADHD symptoms.
A patient can have ADHD and borderline personality disorder. This combination may produce severe emotional dysregulation, rejection sensitivity, impulsive decisions, relationship conflict, task failure and shame. ADHD-related repeated failures can worsen self-esteem, while BPD-related interpersonal sensitivity can intensify emotional crises.
A patient can have bipolar disorder and borderline personality disorder. This is often diagnostically challenging. The clinician must separate sustained hypomanic/manic episodes from rapid interpersonal reactivity.
NIMH notes that BPD often co-occurs with mood disorders, ADHD, PTSD, anxiety, substance use disorders and eating disorders, and that overlapping symptoms can make diagnosis and treatment harder.
10. Assessment approach in clinical practice
A good assessment should not begin with labels. It should begin with a timeline.
A practical structure
First, map the patient’s life chronologically: childhood temperament, school functioning, attention, impulsivity, family environment, trauma, relationships, academic performance, substance use, sleep pattern and occupational history.
Second, identify discrete mood episodes. Ask about periods of elevated or irritable mood with increased energy, decreased need for sleep, overactivity, disinhibition, overspending, sexual risk, grandiosity, increased talking or unusual confidence.
Third, examine emotional triggers. Are shifts mainly interpersonal? Do they occur after perceived rejection, abandonment, criticism, delay, conflict or shame?
Fourth, assess executive function. Has the person always had problems with planning, organising, sustaining attention, completing tasks, regulating time and controlling impulses?
Fifth, obtain collateral history. Family members often clarify whether behaviour was a true departure from baseline.
Sixth, screen for mimics: substance use, antidepressant activation, steroid use, thyroid disease, sleep deprivation, trauma, autism, complex PTSD and personality structure.
Seventh, assess risk carefully: self-harm, suicide, aggression, driving risk, sexual risk, financial risk and vulnerability to exploitation.
For ADHD, NICE recommends assessment of needs, coexisting conditions, social, familial, educational or occupational circumstances and physical health as part of diagnosis.
11. Treatment implications
Bipolar disorder
Treatment usually centres on mood stabilisation, relapse prevention, psychoeducation, sleep regularity, early warning sign monitoring, family involvement and careful management of antidepressants or stimulants. NICE recommends specialist assessment for suspected bipolar disorder and includes pharmacological, psychological, social, occupational and educational interventions in appropriate services.
For mania or hypomania, NICE recommends reducing stimulation, avoiding major decisions until recovery, and using appropriate antipsychotic or mood-stabilising strategies depending on clinical context.
Borderline personality disorder
The foundation is a structured, hopeful, consistent therapeutic approach. The goals are emotional regulation, distress tolerance, interpersonal effectiveness, reduction of self-harm, identity integration and crisis planning.
NICE recommends psychological treatment planning that considers patient preference, severity, motivation, ability to remain within therapeutic boundaries and available support. It also recommends structured care, a clear theoretical approach and therapist supervision.
Medication should not be used as the primary treatment for BPD itself. NICE states that drug treatment should not be used specifically for borderline personality disorder or its individual symptoms such as repeated self-harm, emotional instability, risk-taking behaviour or transient psychotic symptoms; antipsychotics should not be used for medium- or long-term treatment of BPD.
ADHD
Treatment includes psychoeducation, environmental modification, sleep and routine work, coaching-style interventions, CBT-informed strategies, workplace or academic accommodations, and medication when impairment persists.
NICE recommends medication for adults with ADHD when symptoms continue to cause significant impairment after environmental modifications have been implemented and reviewed. It recommends lisdexamfetamine or methylphenidate as first-line pharmacological treatment for adults, with atomoxetine considered when stimulants are not tolerated or ineffective after adequate trials.
12. Common diagnostic traps
Trap 1: Calling every mood swing bipolar
Rapid emotional shifts after rejection, criticism or relational conflict are more suggestive of emotional dysregulation than bipolar disorder, unless accompanied by sustained activation.
Trap 2: Missing bipolar disorder in a patient with depression
Many patients present during depression and do not spontaneously report hypomania. Asking specifically about overactivity, decreased sleep, disinhibition and episodic confidence is essential.
Trap 3: Mistaking adult ADHD for hypomania
Talkativeness, restlessness and distractibility can look like hypomania. The question is whether these are lifelong traits or a distinct episode.
Trap 4: Treating BPD only with medication
Medication may help comorbid depression, anxiety, PTSD, ADHD or bipolar disorder, but it does not replace structured psychotherapy and crisis planning for BPD.
Trap 5: Ignoring comorbidity
A patient may genuinely have more than one condition. The aim is not to force a single label but to identify which symptoms belong to which mechanism.
13. A simple clinical decision rule
When confused, ask three questions:
1. Is there a sustained episode of activation?
Think bipolar disorder.
2. Are the mood shifts rapid, intense and interpersonal?
Think borderline personality structure or trauma-related dysregulation.
3. Have attention, impulsivity, disorganisation and emotional reactivity been present since childhood?
Think ADHD.
Then ask:
Can more than one be true?
In many complex patients, the answer is yes.
Conclusion
Bipolar disorder, borderline personality disorder and ADHD overlap on the surface but differ at the level of time course, triggers, sleep-energy pattern, impulsivity and developmental history.
The most clinically powerful distinction is:
Bipolar disorder is episodic activation.
Borderline personality disorder is relational-emotional lability.
ADHD is lifelong executive dysregulation.
Good diagnosis requires a timeline, collateral history, careful risk assessment and humility. Labels should not be used defensively or pejoratively. They should guide treatment. When the formulation is accurate, patients often feel relieved: their suffering becomes understandable, and treatment becomes more targeted.
When should you seek professional help?
If mood swings, impulsivity, irritability, poor concentration, sleep disturbance, relationship instability or repeated emotional crises are affecting your work, studies, family life or self-esteem, it is better not to self-diagnose. Bipolar disorder, borderline personality disorder and ADHD can overlap, and the wrong label can delay recovery or lead to inappropriate treatment.
A careful psychiatric assessment can help clarify whether the problem is primarily episodic mood activation, emotional dysregulation, ADHD-related executive dysfunction, trauma-related distress, substance-related symptoms, or a combination of these. Once the diagnosis is clearer, treatment can be planned more safely — whether that involves medication, psychotherapy, lifestyle work, family psychoeducation, ADHD-focused strategies, mood stabilisation or structured therapy.
For a detailed assessment and personalised treatment plan, you may consult:
Dr. Srinivas Rajkumar T, MD AIIMS, DNB, MBA
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery
Opp. Phoenix Mall, Chennai
📞 +91-8595155808
✉️ srinivasaiims@gmail.com
Related posts:
- Adult ADHD: Assessment, Diagnosis, Differential Diagnosis, and Treatment
- Why Family Psychoeducation Matters in Bipolar Disorder
- ✅ Autism Screening in Children – When, How & Why Early Diagnosis Matters
- ADHD vs Borderline Personality Disorder in Women: Untangling Two Overlapping Worlds
- The Bottomless Pit: Why You’ll Never Feel ‘Enough’ in Borderline Personality Disorder
- EUPD, Borderline Personality Disorder, Mood Changes, PCOS and Periods: Why Hormonal Patterns Should Not Be Missed