Paranoid Personality Disorder in ICD 11 , DSM 5 , PDM 3
 Long before psychiatry acquired its modern diagnostic language, clinicians were already familiar with a certain kind of person—one who lived in a world subtly, but persistently, tinged with mistrust.
Long before psychiatry acquired its modern diagnostic language, clinicians were already familiar with a certain kind of person—one who lived in a world subtly, but persistently, tinged with mistrust.
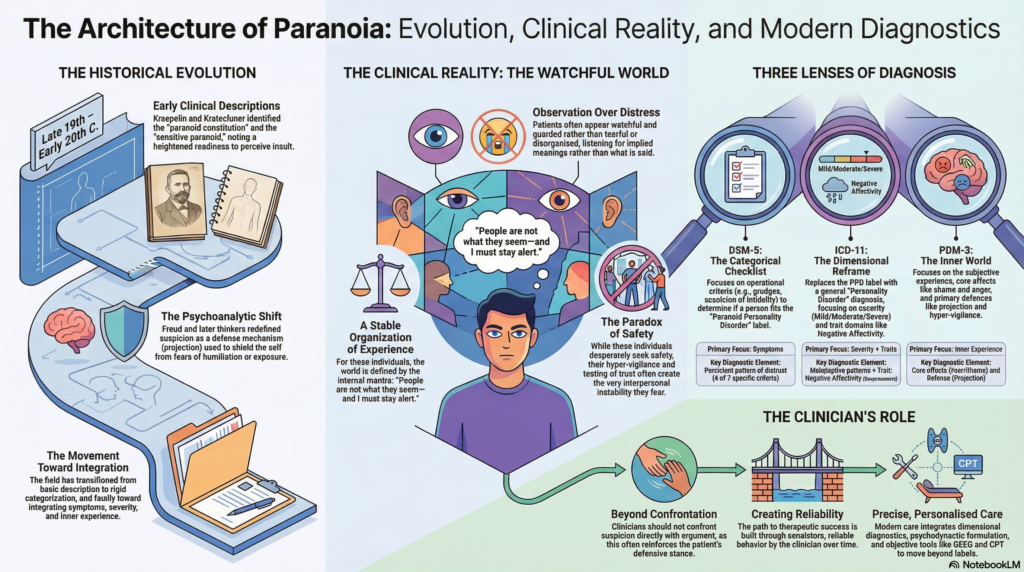
Early psychiatric writings from the late 19th and early 20th centuries described individuals who were “sensitive,” “suspicious,” or “self-referential.” Emil Kraepelin referred to forms of paranoid constitution, while Ernst Kretschmer spoke of the sensitive paranoid personality—individuals whose inner vulnerability coexisted with a heightened readiness to perceive insult or threat.
In psychoanalytic traditions, these observations deepened. Suspicion was no longer seen merely as a trait, but as a defensive organization of the mind. Sigmund Freud conceptualized paranoia in terms of projection—where unacceptable internal feelings were attributed to others. Later thinkers expanded this understanding, recognizing that what appears as hostility toward the world often conceals a profound fear of humiliation or exposure.
With the emergence of modern classificatory systems, there was an effort to standardize these observations. Systems like DSM-III and later DSM-5 translated these rich clinical descriptions into operational diagnostic criteria—lists of observable features aimed at improving reliability.
Yet, something was inevitably lost in this translation.
The inner world—the meaning behind suspicion, the developmental pathways, the emotional undercurrents—was often reduced to checklists. Over time, clinicians began to recognize the limitations of rigid categories.
This led to a rethinking of personality disorders.
The ICD-11 marks a significant shift, moving toward severity and trait-based understanding, while the PDM-3 continues to preserve the depth of subjective experience.
Thus, the story of paranoid personality is also the story of psychiatry itself:
👉 a movement from description → categorization → toward integration.
Entering the Clinical Reality
There is a certain kind of patient who does not walk into the clinic with obvious distress.
They are not overtly anxious.
They are not tearful.
They are not disorganized.
Instead, they are watchful.
They listen carefully—not just to what is said, but to what might be implied. A casual remark may be examined, turned over, and reinterpreted. A delay in response may be felt as intentional. Trust is not given; it must be tested—and even then, it remains provisional.
If one were to summarize their internal world:
👉 “People are not what they seem—and I must stay alert.”
This is not merely suspicion.
It is a stable organization of experience.
DSM-5: Paranoid Personality Disorder as a Defined Category
The DSM-5 retains a categorical approach.
It asks:
👉 Does this person meet criteria?
Core Diagnostic Idea
A pervasive pattern of distrust and suspiciousness, where others’ motives are interpreted as malevolent.
Diagnostic Criteria (Expanded Understanding)
At least four of the following:
- Persistent suspicion of exploitation or harm
- Doubts about loyalty
- Reluctance to confide
- Misinterpretation of benign remarks
- Grudges and unforgiving stance
- Perceived attacks leading to anger
- Suspicion of infidelity
Clinical Presentation
These patients often:
- Maintain emotional distance
- Appear guarded and formal
- Misread interpersonal cues
- React strongly to perceived slights
There is a paradox:
👉 They seek safety, but create instability.
Strengths and Limitations
Strengths
- Clear and operational
- Useful for communication
Limitations
- Rigid categories
- High overlap
- Limited insight into severity and inner experience
ICD-11: A Dimensional Reframing
The ICD-11 removes “paranoid personality disorder” as a separate diagnosis.
Instead, it reframes personality pathology
Step 1: Personality Disorder Diagnosis
Based on:
- Self dysfunction
- Interpersonal dysfunction
- Persistent maladaptive patterns
Step 2: Severity
- Mild
- Moderate
- Severe
Severity predicts:
- Risk
- Prognosis
- Treatment needs
Step 3: Trait Domains
Paranoid traits fall under:
Negative Affectivity
- Suspiciousness
- Hostility
- Emotional sensitivity
Dissociality (sometimes)
- Distrust
- Interpersonal detachment
Clinical Translation
Instead of a label, we describe:
👉 Moderate Personality Disorder with prominent suspiciousness (Negative Affectivity)
Why This Matters
- Reflects clinical reality
- Allows personalised formulation
- Moves beyond artificial categories
PDM-3: The Inner World of Paranoia
The PDM-3 shifts focus inward.
It asks:
👉 What does the world feel like to this person?
Core Experience
A persistent expectation of:
👉 Harm, humiliation, or betrayal
Emotional Core
- Fear
- Shame
- Anger
These are rarely expressed directly.
Defenses
Projection
Internal threat → external attribution
Hypervigilance
Constant scanning for danger
Self-Experience
- Vulnerable but concealed
- Rigid or morally certain outwardly
- Sensitive to criticism
Interpersonal Style
- Testing trust
- Misinterpreting neutrality
- Difficulty with closeness
Levels of Organization
- Neurotic → mild suspiciousness
- Borderline → stress-induced paranoia
Integrating the Models
| System | Focus |
|---|---|
| DSM-5 | Symptoms |
| ICD-11 | Severity + traits |
| PDM-3 | Inner experience |
A Clinical Example
A patient with:
- Persistent distrust
- Misinterpretation of remarks
- Reluctance to confide
DSM-5
✔ Paranoid Personality Disorder
ICD-11
✔ Moderate Personality Disorder
✔ Trait: Negative Affectivity
PDM-3
✔ Paranoid personality pattern
✔ Defense: projection
✔ Core affect: fear of humiliation
Final Reflection
Paranoid personality is not just mistrust.
It is a world where:
- Safety is uncertain
- Intentions are suspect
- Vulnerability feels dangerous
The clinician’s role is not to confront suspicion directly.
👉 It is to create reliability over time.
Not through argument.
But through consistency.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
With a clinical approach that integrates:
- ICD-11 dimensional diagnostics
- Psychodynamic formulation
- Objective tools such as QEEG and CPT
Dr. Srinivas focuses on moving beyond labels toward precise, personalised psychiatric care.