Expressed Emotion in Psychiatry: A Nuanced Exploration of Positive and Negative Dimensions
 Expressed Emotion (EE), over decades, has often been framed in a risk-oriented language—high EE predicts relapse, criticism worsens outcomes, over-involvement destabilizes recovery. While empirically valid, this framing is incomplete.
Expressed Emotion (EE), over decades, has often been framed in a risk-oriented language—high EE predicts relapse, criticism worsens outcomes, over-involvement destabilizes recovery. While empirically valid, this framing is incomplete.
A more mature understanding recognizes that EE is not simply high vs low, but rather:
A spectrum of emotional engagement—where both negative and positive expressions can either heal or harm depending on context, intensity, and timing.
1. Moving Beyond “High EE = Bad”
The classical model categorized families as:
- High EE → criticism, hostility, over-involvement
- Low EE → relative emotional neutrality
However, this dichotomy ignores a crucial reality:
Emotional expression itself is not pathological—dysregulated expression is.
Thus, EE must be understood along two axes:
- Valence → Positive vs Negative
- Regulation → Balanced vs Dysregulated
2. Negative Expressed Emotion: Structure and Meaning
Negative EE includes:
- Criticism
- Hostility
- (Certain forms of) Over-involvement
But these are not merely behaviors—they are emotional communications shaped by meaning.
A. Criticism: The Language of Frustration
At surface:
- “You are not trying hard enough.”
At depth:
- Attribution: Illness = controllable
- Emotion: Frustration, disappointment
Clinical Impact:
- Amplifies self-criticism in depression
- In schizophrenia, increases paranoid interpretations
- In OCD, worsens guilt and intrusive thought distress
Subtle Insight:
Criticism often reflects a caregiver’s failure to metabolize uncertainty
B. Hostility: The Breakdown of Empathy
Hostility represents:
- Global rejection of the patient
- Collapse of distinction between person and illness
Example:
- “He is impossible as a person.”
Clinical Impact:
- Erodes therapeutic alliance at home
- Increases shame and identity fragmentation
- Strong predictor of relapse across disorders
Deeper Layer:
Hostility frequently emerges from chronic caregiver burnout
C. Emotional Over-Involvement (EOI): Care that Overflows Boundaries
EOI is the most misunderstood component.
It includes:
- Overprotection
- Excessive sacrifice
- Intrusive monitoring
Dual Nature:
| Adaptive Form | Pathological Form |
|---|---|
| Supportive presence | Intrusive control |
| Availability | Enmeshment |
| Advocacy | Loss of autonomy |
Clinical Impact:
- Inhibits self-efficacy
- Reinforces illness identity
- In bipolar disorder → destabilizes recovery during euthymia
Core Insight:
EOI is often anxiety disguised as love
3. Positive Expressed Emotion: The Underemphasized Protective Field
Modern psychiatry increasingly emphasizes the protective dimensions of EE, which were historically under-theorized.
Positive EE includes:
- Warmth
- Positive remarks
- Emotional attunement
A. Warmth: The Regulator of Psychological Safety
Warmth is not sentimentality—it is:
- Emotional availability
- Non-judgmental presence
- Recognition of the patient’s subjective experience
Clinical Effects:
- Reduces stress reactivity
- Improves treatment adherence
- Enhances self-esteem regulation
Neurobiological Correlates:
- Lower cortisol responses
- Better prefrontal modulation of emotional circuits
Key Insight:
Warmth provides a holding environment in the Winnicottian sense
B. Positive Remarks: Micro-Affirmations
These are small but powerful:
- “You handled that well.”
- “I can see you are trying.”
Clinical Effects:
- Reinforces adaptive behavior
- Counters cognitive distortions
- Builds resilience over time
Subtle Distinction:
- Genuine vs performative positivity
- Specific vs vague praise
C. Attuned Involvement: The Ideal Middle Ground
The most therapeutic form of EE is:
Involvement that is responsive, not intrusive
Characteristics:
- Respects autonomy
- Offers support when needed
- Withdraws when appropriate
This is essentially:
- Secure attachment in action
4. Dynamic Interplay: Positive and Negative EE Coexist
Families rarely exhibit “pure” forms.
A typical pattern:
- High warmth + high criticism
- High involvement + fluctuating hostility
Thus:
The pattern, rhythm, and context of EE matter more than isolated behaviors
Example:
- Occasional criticism within a warm relationship → tolerable
- Criticism within a hostile environment → pathogenic
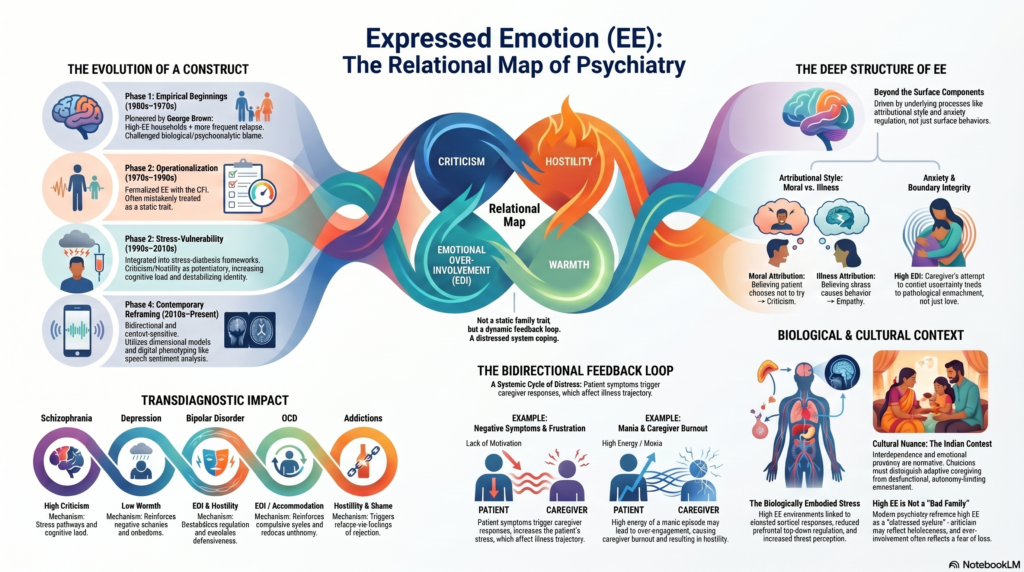
5. Evolution of EE: Toward a Systems Model
From early work by George Brown, EE has evolved:
Earlier View:
- Static family trait
- Predictor of relapse
Modern View:
- Dynamic relational process
- Bidirectional:
- Patient symptoms influence EE
- EE influences symptom trajectory
Systems Perspective:
EE is part of a self-regulating emotional system within the family
6. Cultural Nuances: Reframing Positive and Negative EE in India
In Indian families:
- High involvement is normative
- Emotional expression is often intense but relationally embedded
Important distinctions:
- Warmth may coexist with control
- Criticism may be culturally normalized
Clinical Challenge:
Distinguish between cultural idioms of care and pathological emotional climates
7. Clinical Implications: Working with Both Sides of EE
Traditional Goal:
- Reduce high EE
Modern Goal:
- Rebalance emotional expression
A. Addressing Negative EE
- Reframe illness attribution
- Reduce blame narratives
- Manage caregiver burnout
B. Enhancing Positive EE
- Encourage:
- Specific positive feedback
- Emotional validation
- Build reflective capacity in caregivers
C. Regulating Involvement
- Shift from:
- Control → Collaboration
- Intrusion → Availability
8. A More Refined Clinical Formulation
Instead of labeling a family as “high EE,” a more nuanced formulation would include:
- Attribution style (blame vs illness understanding)
- Emotional tone (hostile, anxious, warm)
- Boundary pattern (detached, enmeshed, balanced)
- Regulatory capacity (reactive vs reflective)
9. The Deeper Psychiatric Insight
EE ultimately reflects something fundamental:
How humans respond to suffering in those they love
- Some respond with control
- Some with withdrawal
- Some with attuned presence
Thus, EE is not just a clinical variable—it is a window into relational adaptation under stress.
Conclusion: Toward an Integrative View
Expressed Emotion should no longer be seen as merely a risk factor to be minimized, but as:
A relational field to be understood, regulated, and transformed
Where:
- Negative EE signals distress and dysregulation
- Positive EE represents healing potential
The task of the clinician is not to silence emotion, but to shape it into a form that supports recovery rather than undermines it.
For Clinical Practice & Consultation
In patients with recurrent relapses, treatment resistance, or complex interpersonal dynamics, a nuanced analysis of both positive and negative Expressed Emotion can significantly refine management strategies.
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
Related posts:
- Stopping Escitalopram (Nexito): A Nuanced, Evidence-Informed Patient Guide
- AI and Emotion Recognition: Understanding Human Feelings Through Technology
- Patterned rTMS: Theta Burst Stimulation and Quadri-Pulse Stimulation – A Detailed Exploration
- 🩺 DBT Emotion Regulation Skills: PLEASE & ABC PLEASE
- Phenocopy of Autism: A QEEG Exploration and Revelation
- QEEG-Led Clinical Breakthrough: Primary vs Secondary Negative Symptoms in Schizophrenia