Redesigning Psychosis Management: The Future of Schizophrenia Treatment
 Schizophrenia has long been one of the most serious and misunderstood psychiatric disorders. For decades, treatment has been dominated by antipsychotic medication, risk management, family psychoeducation, and social rehabilitation. These remain essential. But psychiatry is now standing at an important turning point.
Schizophrenia has long been one of the most serious and misunderstood psychiatric disorders. For decades, treatment has been dominated by antipsychotic medication, risk management, family psychoeducation, and social rehabilitation. These remain essential. But psychiatry is now standing at an important turning point.
Recent advances in neurobiology, psychopharmacology, immunology, biomarkers, digital health, artificial intelligence, and psychotherapy are beginning to reshape how we understand and manage psychosis. The future of schizophrenia treatment will not be a simple replacement of old treatments with new ones. Rather, it will be a redesign of the entire care model — from symptom control to precision, prevention, recovery, and meaningful community reintegration.
A recent article by Bernard R. Bukala, Redesigning psychosis management: future of schizophrenia treatments, argues that schizophrenia care can serve as a useful model for the future of psychiatry itself. The article highlights how pharmacology, biomarkers, psychotherapy, digital tools, and multidisciplinary care may together create a new generation of psychosis services.
The Old Model: Dopamine, Antipsychotics, and Symptom Control
Since the 1950s, antipsychotic medication has been the foundation of schizophrenia treatment. These medicines have transformed psychiatric practice. They reduce hallucinations, delusions, agitation, relapse risk, and the need for prolonged institutional care. For many patients, antipsychotics make the difference between repeated crises and a stable life.
However, the old model has limitations.
Most antipsychotics primarily target positive symptoms — delusions, hallucinations, suspiciousness, disorganised thinking, and behavioural disturbance. Their effect on negative symptoms such as avolition, anhedonia, emotional blunting, and social withdrawal is often modest. Their effect on cognitive symptoms such as poor attention, working memory deficits, and executive dysfunction is also limited.
This is a major issue because, in real-world functioning, negative and cognitive symptoms often determine long-term disability more than hallucinations or delusions alone.
A patient may no longer hear voices, but may still struggle to study, work, initiate activities, maintain relationships, or plan daily life. This is why the future of schizophrenia treatment must go beyond “reducing psychosis” and move toward restoring function, identity, autonomy, and quality of life.
Moving Beyond Dopamine-Centric Psychiatry
For many years, schizophrenia was explained mainly through the dopamine hypothesis. Dopamine dysregulation, particularly striatal hyperdopaminergia, remains highly relevant. But the newer understanding is much broader.
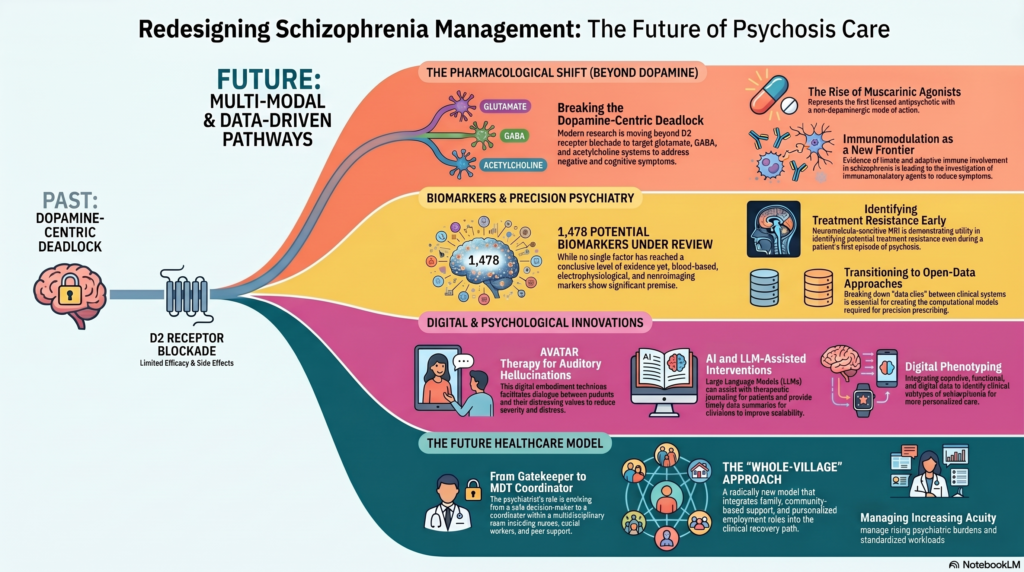
The article highlights a shift from dopamine-only explanations toward a network-level understanding of psychosis. Glutamate, GABA, acetylcholine, serotonin, immune pathways, metabolic systems, and neurodevelopmental mechanisms are increasingly recognised as important contributors.
One important model suggests that reduced cortical glutamate activity may weaken inhibitory GABAergic control, resulting in disinhibition of striatal dopamine neurons. In simpler terms, schizophrenia may involve a cascade of circuit-level disturbances rather than one isolated neurotransmitter abnormality.
This matters clinically because treatment development is also changing. Future antipsychotics may not simply block dopamine D2 receptors. They may modulate glutamate, GABA, acetylcholine, inflammatory pathways, or broader brain circuits.
Xanomeline-Trospium and the Arrival of Non-Dopaminergic Antipsychotics
One of the most important recent developments is the emergence of xanomeline-trospium, also known as KarXT. It is described in the article as the first antipsychotic with a primarily non-dopaminergic mechanism of action to be licensed. Instead of directly blocking dopamine receptors, it acts through muscarinic acetylcholine receptors.
This is conceptually important.
For decades, almost every effective antipsychotic had some relationship with dopamine D2 receptor blockade. KarXT suggests that psychosis can be treated through other neurochemical routes. This opens the possibility of future medicines that may reduce psychosis with fewer extrapyramidal, prolactin-related, or metabolic adverse effects — although real-world safety and long-term data will still be important.
This development also encourages a broader question: instead of asking “Which dopamine blocker should we use?”, future psychiatry may ask, “Which biological pathway is most relevant in this patient?”
That is the beginning of precision psychiatry.
Clozapine: Still the Gold Standard for Treatment Resistance
Despite newer developments, clozapine remains irreplaceable in treatment-resistant schizophrenia. The article notes that clozapine is the only antipsychotic shown to be more effective in treatment-resistant cases.
This is a crucial clinical point. Many patients remain unwell for years because clozapine is delayed, avoided, or underused due to fear of monitoring requirements and side effects. But untreated treatment-resistant psychosis carries its own burden: repeated admissions, family exhaustion, disability, self-neglect, violence risk in a minority, suicide risk, and social deterioration.
The future of schizophrenia care should not neglect clozapine while chasing newer drugs. Instead, we need better systems for safe clozapine initiation, monitoring, adherence support, side-effect management, and patient education.
Clozapine also teaches us a larger lesson. Its superior efficacy may not come from simple dopamine blockade alone. Its effects on serotonin, acetylcholine, glutamate, and broader neurobiological systems remind us that schizophrenia is not a single-pathway disorder.
Immunology and the Inflammation Frontier
Another important future direction is the immune system. The article highlights increasing evidence for involvement of both innate and adaptive immunity in schizophrenia. Immunomodulation is now considered an important frontier in drug development.
This does not mean schizophrenia is simply an inflammatory disease. It means that, in at least a subgroup of patients, immune dysregulation may contribute to symptom onset, progression, or treatment resistance.
This has important implications.
In the future, we may identify inflammatory subtypes of psychosis. Some patients may benefit from adjunctive anti-inflammatory or immunomodulatory approaches. Others may not. This again points toward the need for biomarkers and careful stratification.
The danger is overgeneralisation. Not every patient with schizophrenia needs immune treatment. But the opportunity is equally important: some patients who currently fall into the vague category of “poor response” may actually belong to a biologically distinct subgroup.
Biomarkers: Promise, But Not Yet Routine Clinical Reality
Psychiatry has long lacked reliable biomarkers. Unlike diabetes, where glucose and HbA1c guide treatment, or cardiology, where ECG, troponin, echocardiography, and lipid markers shape decisions, schizophrenia diagnosis still depends mainly on clinical history and mental status examination.
The article discusses a large umbrella review that examined 1,478 potential biomarkers across more than 390,000 participants. Importantly, none had conclusive evidence yet. However, several areas showed promise, including blood-based markers, auditory event-related potentials such as P300 latency, and neuroimaging measures like ventricle-brain ratio.
This is a balanced message. Biomarkers are promising, but they are not yet ready to replace clinical judgment.
Future biomarkers may help in four major ways:
First, they may identify people at high risk before full-blown psychosis develops.
Second, they may predict which patients are likely to respond to standard antipsychotics.
Third, they may help identify treatment-resistant schizophrenia earlier.
Fourth, they may separate schizophrenia into biological subtypes rather than relying only on symptom clusters.
But this future requires strong data systems, replication, ethical safeguards, affordability, and clinical usability. A biomarker that is statistically significant in research but impractical in a busy clinic will not change patient care.
Digital Phenotyping and Precision Psychiatry
A particularly interesting direction is digital phenotyping. This means using data from smartphones, wearables, cognitive tests, speech patterns, sleep rhythms, activity levels, and ecological momentary assessments to understand a patient’s real-life functioning.
The article mentions that integrating cognitive, functional, and digital phenotyping may help identify clinically useful subtypes in schizophrenia.
This is highly relevant to future psychiatric practice.
Currently, follow-up visits often depend on patient recall and family report. A patient may say, “I am fine,” while sleep has reduced, activity has declined, suspiciousness has increased, and social withdrawal has worsened. By the time relapse is obvious, the window for early intervention may have been missed.
Digital monitoring could detect subtle relapse signatures earlier: reduced mobility, disturbed sleep, increased phone inactivity, social rhythm disruption, or changes in speech. Used ethically, this can help clinicians intervene before hospitalisation becomes necessary.
But digital psychiatry must be humane. Patients should not feel surveilled. Consent, privacy, transparency, and data ownership are central. Technology should support trust, not replace it.
Psychological Therapies: Beyond Medication Alone
Schizophrenia treatment is incomplete without psychological therapies. Cognitive Behavioural Therapy for Psychosis, or CBT-P, is one of the best-studied approaches. It can help patients understand voices, reduce distress, evaluate beliefs, manage triggers, and improve coping.
However, the article also notes that CBT-P has mixed evidence. Some trials show benefit, but effects may fade over time, and not all studies demonstrate clear improvement.
This should not be seen as failure. Instead, it suggests that psychological therapy for psychosis needs refinement, personalisation, and continuity.
A patient who hears voices may not only need symptom reduction. They may need help with shame, fear, trauma, social defeat, self-stigma, family conflict, unemployment, and loss of identity. Psychotherapy must therefore move beyond “challenging delusions” and toward rebuilding agency.
AVATAR Therapy and Digital Psychotherapy
One of the most fascinating innovations mentioned in the article is AVATAR therapy. In this approach, a digital representation of a distressing voice is created, allowing the patient to engage in a controlled therapeutic dialogue with it. This can reduce the power, distress, and emotional impact of auditory hallucinations.
This is a powerful example of how technology can enhance therapy.
For many patients, voices are experienced as dominant, threatening, humiliating, or persecutory. AVATAR therapy externalises the voice in a structured way, allowing the patient to gradually shift from fear to mastery.
Other digital interventions mentioned include tools for symptom management, relapse prevention, monitoring, and therapy delivery. The article refers to digital health technologies such as AVATAR therapy, SloMo, and CareLoop being reviewed by NICE in the UK.
In the Indian context, such tools may not immediately be available everywhere. But the principle is important: digital tools can extend care between appointments, support relapse prevention, and make therapy more accessible.
The Role of AI and Large Language Models
The article also points toward the possible role of artificial intelligence and large language models in future psychosis care — for example, LLM-assisted journaling for patients or AI-generated summaries for clinicians.
This is a promising but sensitive area.
AI could help patients track symptoms, structure thoughts, practise coping skills, and prepare for appointments. For clinicians, AI could summarise longitudinal data, identify relapse patterns, organise family reports, and support documentation.
But AI must not become a substitute for clinical responsibility. In psychosis, misinterpretation, paranoia, suggestibility, and risk issues require human sensitivity. AI tools should be carefully governed, clinically validated, and used as assistive systems — not autonomous therapists.
The future psychiatrist may need to become both a clinician and a data interpreter: someone who can combine phenomenology, neuroscience, family context, digital signals, and ethical judgment.
Multidisciplinary Care: From Psychiatrist-Centred to Whole-Village Care
The future of schizophrenia treatment is not only about new medicines or biomarkers. It is also about redesigning services.
The article argues that psychiatrists are no longer sole gatekeepers of treatment. They are increasingly coordinators within multidisciplinary teams that include nurses, psychologists, social workers, occupational therapists, employment advisors, peer workers, families, and community systems.
This is especially important in schizophrenia.
Medication may reduce hallucinations, but recovery requires much more: family support, vocational rehabilitation, cognitive remediation, substance-use intervention, sleep regulation, physical health monitoring, social skills training, and stigma reduction.
A “whole-village” model means that care extends beyond the prescription pad. It involves the family, workplace, educational institution, community, digital support systems, and primary care physicians.
For India, this is particularly relevant. Families often provide the majority of long-term care. Instead of treating families as passive bystanders, future services should train, support, and empower them.
Physical Health Cannot Be Ignored
One of the biggest tragedies in schizophrenia care is the physical health gap. Patients with schizophrenia have higher rates of diabetes, obesity, dyslipidaemia, smoking, cardiovascular disease, and reduced life expectancy.
Antipsychotic-related cardiometabolic burden is specifically highlighted in the article as one of the major limitations of current treatment.
Future psychosis care must therefore integrate physical health from the beginning. Weight, waist circumference, blood pressure, fasting glucose, HbA1c, lipids, liver function, prolactin, movement disorders, sleep, diet, and exercise should not be afterthoughts.
A good schizophrenia clinic of the future should look partly like a brain clinic, partly like a metabolic clinic, partly like a rehabilitation centre, and partly like a family-support system.
Early Detection and Prevention
The article also discusses the importance of risk stratification and early detection. The goal is to bring therapeutic intervention closer to illness onset.
This is critical because duration of untreated psychosis is associated with poorer outcomes. Early recognition can prevent academic decline, occupational failure, family disruption, self-harm, and social deterioration.
However, early detection must be handled carefully. Labelling someone as “high risk” for psychosis can create anxiety and stigma. Not everyone with attenuated symptoms develops schizophrenia. Therefore, early intervention models must be ethical, non-stigmatising, and proportionate.
The ideal model is not fear-based prediction. It is supportive monitoring, stress reduction, substance-use prevention, family education, sleep stabilisation, and early treatment when clearly needed.
The Indian Context: What Needs to Change?
In India, schizophrenia care faces unique challenges. These include stigma, delayed help-seeking, faith-healing pathways, irregular follow-up, medication discontinuation, caregiver burnout, limited rehabilitation services, and shortage of trained mental health professionals.
At the same time, India has strengths: strong family involvement, growing mental health awareness, expanding digital access, and increasing psychiatric training capacity.
The future Indian psychosis-care model should include:
A structured first-episode psychosis pathway.
Early and rational antipsychotic use.
Timely clozapine initiation in treatment resistance.
Family psychoeducation as a routine intervention.
Digital relapse monitoring where feasible.
Affordable cognitive and functional assessment.
Vocational rehabilitation partnerships.
Metabolic monitoring built into every clinic visit.
Community-based follow-up using trained mental health workers.
Clear anti-stigma communication in schools, colleges, workplaces, and media.
This is where psychiatry can evolve from episodic crisis care to longitudinal recovery care.
From “Chronic Illness” to “Recovery-Oriented Care”
Schizophrenia is often described as a chronic brain disorder. While this may be scientifically useful, it can sound discouraging to patients and families. A more balanced message is needed.
Schizophrenia is a serious psychiatric disorder. It can be disabling. It requires long-term care. But it is also treatable. Many patients improve substantially. Many can study, work, marry, parent, create, and contribute meaningfully to society.
Recovery does not always mean complete absence of symptoms. It means regaining direction, dignity, relationships, purpose, and self-management.
The future of schizophrenia care must be optimistic without being unrealistic, scientific without being cold, and technologically advanced without becoming impersonal.
Conclusion: The Future Is Integrated, Personalised, and Humane
The future of schizophrenia treatment will not come from one miracle drug or one digital app. It will come from integration.
Antipsychotics will remain important, but pharmacology will move beyond dopamine. Clozapine will remain essential, but treatment resistance may be detected earlier. Biomarkers may not yet be ready for routine care, but they are moving psychiatry toward precision. Digital tools may support monitoring and therapy, but they must be governed ethically. Psychological therapies will become more personalised. Families and multidisciplinary teams will become central to recovery.
The most important change will be philosophical.
Schizophrenia management must move from a narrow model of symptom suppression to a broader model of brain-based, person-centred, recovery-oriented care.
The future psychiatrist will not merely prescribe medication. The future psychiatrist will integrate neuroscience, phenomenology, biomarkers, digital data, psychotherapy, family systems, physical health, and social rehabilitation.
That is the real redesign of psychosis management.
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808